
Abstract 摘要
Myopia, also known as short-sightedness or near-sightedness, is a very common condition that typically starts in childhood. Severe forms of myopia (pathologic myopia) are associated with a risk of other associated ophthalmic problems. This disorder affects all populations and is reaching epidemic proportions in East Asia, although there are differences in prevalence between countries. Myopia is caused by both environmental and genetic risk factors. A range of myopia management and control strategies are available that can treat this condition, but it is clear that understanding the factors involved in delaying myopia onset and slowing its progression will be key to reducing the rapid rise in its global prevalence. To achieve this goal, improved data collection using wearable technology, in combination with collection and assessment of data on demographic, genetic and environmental risk factors and with artificial intelligence are needed. Improved public health strategies focusing on early detection or prevention combined with additional effective therapeutic interventions to limit myopia progression are also needed.
近视,也称为近视或近视,是一种非常常见的疾病,通常始于儿童期。严重形式的近视(病理性近视)与其他相关眼科问题的风险相关。这种疾病影响所有人群,在东亚正达到流行病的程度,尽管各国之间的流行率存在差异。近视是由环境和遗传风险因素共同造成的。有一系列近视管理和控制策略可以治疗这种疾病,但很明显,了解延迟近视发作和减缓其发展所涉及的因素将是降低其全球患病率快速上升的关键。为了实现这一目标,需要利用可穿戴技术改进数据收集,同时收集和评估关于人口、遗传和环境风险因素的数据,并利用人工智能。还需要改进公共卫生策略,侧重于早期检测或预防,结合额外的有效治疗干预,以限制近视的发展。
Similar content being viewed by others
其他人正在查看的类似内容
Introduction 介绍
Myopia (also known as short-sightedness or near-sightedness) is a common condition that develops primarily during childhood and early adulthood when excessive elongation of the eye results in images of distant objects coming into focus in front of the retina, resulting in blurred distance vision. Myopia is one of the most common eye diseases globally1,2,3, with a prevalence of 10–30% in the adult population in many countries and 80–90% in young adults in some parts of East and Southeast Asia.
近视(也称为近视或近视)是一种常见的疾病,主要发生在儿童期和成年早期,此时眼睛过度拉长导致远处物体的图像在视网膜前聚焦,导致远视模糊。近视是全球 1,2,3 最常见的眼病之一,在许多国家的成年人口中患病率为10-30%,在东亚和东南亚的一些地区的年轻人中患病率为80-90%。
Most cases of myopia are associated with excessive axial eye growth4 but some rarer forms can result from disproportionately high corneal power. For example, keratoconus (in which there is progressive thinning of the cornea leading to the formation of a cone-shaped bulge in the cornea) can lead to severe myopia; however, the global prevalence of keratoconus is low (~138 per 100,000 individuals)5. Myopia can also be caused by nuclear cataracts in adults aged 50 years or older. These corneal and lenticular forms of myopia are aetiologically distinct from common axial myopia, have different risk factors and require different approaches to prevention and clinical management; thus, this Primer focuses on axial myopia (Fig. 1).
大多数近视病例与0#时眼轴过度生长有关,但一些罕见的形式可能是由不成比例的高角膜屈光力引起的。例如,圆锥角膜(其中角膜进行性变薄导致角膜中锥形凸起的形成)可导致严重近视;然而,圆锥角膜的全球患病率较低(约每10万人138例) 5 。50岁或以上的成年人也可能由核性白内障引起近视。这些角膜和晶状体形式的近视在病因上不同于普通的轴性近视,具有不同的危险因素,并且需要不同的预防和临床管理方法;因此,该初级读本集中于轴性近视(图1)。
图1:近视的眼形变化。

Light enters an emmetropic eye (+2.00 D to −0.25 D) through various components, including the cornea and the lens, followed by the vitreous, to arrive focused on the retina where signals are processed and transmitted via the optic nerve to the brain for further visual processing. In myopia, light is not correctly refracted, therefore producing images that are focused in front of the retina, leading to blurred vision for objects that are at a distance. This defocus can arise as a result of excessive refraction from anterior structures such as the cornea and lens of the eye, but most cases are caused by abnormal elongation of the eyeball (known as axial myopia). The level of myopia is typically quantified as the spherical equivalent refractive error in dioptres but can also be based on the measurement of axial length in millimetres. A more negative refractive error signifies more severe myopia. Pathologic myopia is a severe form of myopia, in which there is a very high risk of ocular complications such as macular haemorrhage or macular atrophy.
光线通过各种组件进入正视眼(+2.00 D至0.25 D),包括角膜和晶状体,然后是玻璃体,聚焦在视网膜上,信号在视网膜上进行处理,并通过视神经传输到大脑进行进一步的视觉处理。在近视中,光线没有被正确折射,因此产生的图像聚焦在视网膜前面,导致对远处物体的视觉模糊。这种散焦可能是由于眼睛的角膜和晶状体等前部结构的过度折射造成的,但大多数情况下是由眼球的异常伸长引起的(称为轴性近视)。近视的水平通常被量化为以屈光度为单位的球面等效屈光不正,但是也可以基于以毫米为单位的轴长的测量。更负的屈光不正意味着更严重的近视。病理性近视是近视的一种严重形式,其中存在非常高的眼部并发症风险,例如黄斑出血或黄斑萎缩。
Compelling evidence from multiple studies supports the involvement of both nature (genetics and heredity) and nurture (environment and lifestyle) in causing myopia. For most individuals with myopia, the critical causative factor most likely relates to a modern lifestyle, which includes long periods of time spent on educational and other near-work activities. However, genetic factors also have an equally decisive role in conferring different levels of susceptibility to these lifestyle risk factors.
来自多项研究的令人信服的证据支持自然(遗传和遗传)和后天(环境和生活方式)都参与导致近视。对于大多数近视患者来说,关键的致病因素很可能与现代生活方式有关,包括长时间从事教育和其他近距离工作活动。然而,遗传因素在赋予这些生活方式风险因素不同程度的易感性方面也具有同样决定性的作用。
Myopia is defined by a spherical equivalent (SE) ≤−0.5 dioptres (D). Myopia can typically be corrected with glasses, contact lenses or refractive surgery to provide good visual acuity. Any level of myopia can increase the risk of adverse ocular tissue changes but the risk of these effects increases dramatically at high levels of myopia (high myopia, SE worse than −5.0 D or −6.0 D) and in pathologic myopia (pathological retinal changes secondary to high myopia), leading to uncorrectable visual impairment or blindness, including sight-threatening diseases such as glaucoma, retinal detachment and macular holes6.
近视由球面当量(SE)≤0.5屈光度(D)定义。近视通常可以通过眼镜、隐形眼镜或屈光手术来矫正,以提供良好的视力。任何程度的近视都会增加不良眼组织变化的风险,但在高度近视(高度近视,SE比5.0 D或6.0 D差)和病理性近视(继发于高度近视的病理性视网膜变化)中,这些影响的风险会显著增加,导致不可矫正的视力障碍或失明,包括威胁视力的疾病,如青光眼、视网膜脱离和黄斑裂孔 6 。
Rapid increases in the prevalence of all levels of myopia in the past three decades have led to its description as an ‘epidemic’. Accordingly, there has been a push to better understand the risk factors of myopia and to view this condition as a major public health problem. This development reflects the challenges posed by the need to provide optical correction to a large section of the population as well as the need to manage the visual impairment and blindness associated with pathologic myopia. Additionally, primary preventive measures to stop or delay the onset of myopia in children as well as secondary preventive measures to slow the gradual worsening (progression) of myopia during late childhood are being employed.
在过去的三十年中,各种程度的近视患病率的快速增加导致其被描述为一种“流行病”。因此,人们一直在推动更好地了解近视的风险因素,并将这种情况视为一个主要的公共健康问题。这一发展反映了为大部分人口提供光学矫正的需要以及管理与病理性近视相关的视力损害和失明的需要所带来的挑战。此外,正在采用阻止或延迟儿童近视发作的初级预防措施以及减缓儿童晚期近视逐渐恶化(发展)的二级预防措施。
This Primer covers the growing prevalence of myopia in the world, its known environmental and genetic risk factors and how they might contribute to excessive eye growth and myopia, and also updates the current management strategies, including prevention and optical, pharmacological and surgical interventions.
这本初级读本涵盖了近视在世界上日益增长的流行,其已知的环境和遗传风险因素,以及它们如何可能导致眼睛过度生长和近视,还更新了当前的管理策略,包括预防和光学,药物和手术干预。
Epidemiology 流行病学
Regional differences in prevalence
流行率的区域差异
The global prevalence of myopia is almost 2 billion individuals (28.3% of the global population), which includes 277 million individuals (4.0% of the global population) with high myopia7. The prevalence is estimated to increase to 4.76 billion individuals (49.8% of the global population) for myopia and almost 1 billion individuals (9.8% of the global population) for high myopia by 2050 (ref.7). Genetic predisposition has not substantially changed in the past few decades and the rise in myopia prevalence is possibly related to environmental factors such as an increase in the number of years of education, more near-work and reduced time outdoors (see Mechanisms/pathophysiology, below)8,9,10,11,12,13. One of the most striking features of myopia is the high prevalence of both myopia and high myopia in some locations in East and Southeast Asia (47.0%), which is much higher than that in Central Europe (27.1%), Central Asia (17.0%) and Central Africa (7.0%)7. In particular, myopia prevalence is highest in urbanized areas of East and Southeast Asia such as Singapore14, cities in mainland China15, Hong Kong16, Taiwan17,18, Japan19 and South Korea20. By contrast, in regions with less-intensive education systems, the prevalence of myopia is much lower (for example, Lao People’s Democratic Republic, southern Indian states and Morocco)21,22,23.
近视的全球患病率几乎为20亿人(占全球人口的28.3%),其中包括2.77亿高度近视的人(占全球人口的4.0%) 7 。据估计,到2050年,近视的患病率将增加到47.6亿人(占全球人口的49.8%),高度近视的患病率将增加到近10亿人(占全球人口的9.8%)(参考文献。 7 ).遗传易感性在过去几十年中没有实质性变化,近视患病率的上升可能与环境因素有关,如受教育年限的增加、更多的近距离工作和户外时间的减少(见下文机制/病理生理学) 8,9,10,11,12,13 。近视最显著的特征之一是东亚和东南亚部分地区近视和高度近视的患病率较高(47.0%),远高于中欧(27.1%)、中亚(17.0%)和中非(7.0%) 7 。特别是,近视患病率在东亚和东南亚的城市化地区最高,如新加坡 14 、mainland China城市 15 、香港 16 、台湾 17,18 、日本 19 和南韩 20 。相比之下,在教育系统不太密集的地区,近视的患病率要低得多(例如,老挝人民民主共和国、印度南部各邦和摩洛哥) 21,22,23 。
The highest prevalence of myopia in schoolchildren has been reported in urban areas of Asia, including China, Taiwan, South Korea, Singapore and Japan19,24,25. In contrast to rural areas, urban areas have high economic development and educational standards as well as fewer opportunities for children to spend time outdoors. The prevalence in 12-year-old children shows major differences in some Asian regions, with 53.1% in Hong Kong26 and 49.7% in Guangzhou, China15, compared with 20.0% in the USA27 and 11.9% in Australia28. By contrast, the prevalence of myopia remains low in children in some parts of the world, such as in Saudi Arabia (0.7%)29, South America (1.4%)30, Cambodia (6.0%)31, urban India (9.7%)32 and Nepal (16.5%)33.
据报道,亚洲城市地区的学龄儿童近视患病率最高,包括中国、台湾、韩国、新加坡和日本 19,24,25 。与农村地区相比,城市地区的经济发展和教育水平较高,儿童户外活动的机会较少。12岁儿童的患病率在一些亚洲地区显示出重大差异,香港为53.1% 26 ,中国广州为49.7% 15 ,而美国为20.0% 27 ,澳大利亚为11.9% 28 。相比之下,在世界一些地区,儿童近视的患病率仍然很低,如沙特阿拉伯(0.7%) 29 、南美(1.4%) 30 、柬埔寨(6.0%) 31 、印度城市(9.7%) 32 和尼泊尔(16.5%) 33 。
In young adults, the prevalence of myopia has reached >80% in urbanized Asian regions. A very high prevalence has been reported in South Korea (96.5% in those 19 years of age)34, Taiwan (86.1% in those 18–24 years of age)35 and Hong Kong (72.2% in those <35 years of age)16. By contrast, a generational change exists in middle-aged and elderly adults, with a lower myopia prevalence of 19.4% in adults >65 years of age in Taiwan36 and of 22.9% in adults in China (40–90 years of age)37. Prevalence is lower in regions outside of Asia such as the USA (33.1% in individuals >20 years of age)38, Norway (35.0% in individuals 20–25 years of age)39 and Israel (28.3% in those 16–22 years of age)40. Indeed, in Europe, data collected by the European Eye Epidemiology (E3) consortium between 1990 and 2013 indicate that the prevalence of myopia has increased from 17.8% in those born between 1910 and 1939 to 23.5% in those born between 1940 and 1979 (ref.41).
在年轻人中,近视的患病率在亚洲城市化地区已经达到80%以上。据报道,韩国(19岁人口为96.5%) 34 、台湾(18-24岁人口为86.1%) 35 和香港(35岁以下人口为72.2%) 16 的流行率非常高。相比之下,中老年人存在代际变化,台湾>65岁成年人的近视患病率较低,为19.4% 36 ,中国成年人(40-90岁)为22.9% 37 。亚洲以外地区的患病率较低,如美国(20岁以上人群为33.1%) 38 、挪威(20-25岁人群为35.0%) 39 和以色列(16-22岁人群为28.3%) 40 。事实上,在欧洲,欧洲眼流行病学(E 3 )联盟在1990年至2013年间收集的数据表明,近视的患病率从1910年至1939年出生的人的17.8%上升到1940年至1979年出生的人的23.5%(参考文献。 41 ).
High myopia 高度近视
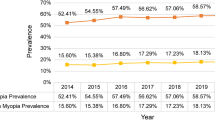
The prevalence of high myopia in urban Asian regions has increased from <10% 10–15 years ago to ~10–20% in Korea34, Taiwan35, Japan19 and several parts of China42,43,44 (Fig. 2). By contrast, the prevalence of high myopia in non-Asian regions is comparatively low, with a prevalence of 2.7% according to data from the E3 consortium in individuals between 25 and 90 years of age45, 0.3% in individuals in Denmark with an average age of 19.3 years46, 1.9% in 17 year olds in Australia47, 2.0% and 2.3% in men and women aged 16–22 years, respectively, in Israel40, and 3.92% in the USA48 (Fig. 2). The prevalence of high myopia in adults ≥40 years of age is 5.7% in Japan49, 5.0% in those ≥40 years of age in Singapore, 4.2% in those ≥65 years of age in Taiwan50 and 2.7% in those ≥49 years of age in Australia51.
亚洲城市地区高度近视的患病率从10-15年前的<10%增加到韩国 34 、台湾 35 、日本 19 和中国部分地区 42,43,44 的~10-20%(图2)。相比之下,非亚洲地区高度近视的患病率相对较低,根据E 3 联盟的数据,25至90岁个体的患病率为2.7% 45 ,平均年龄为19.3岁的丹麦个体的患病率为0.3% 46 ,澳大利亚17岁个体的患病率为1.9% 47 ,16-22岁男性和女性的患病率分别为2.0%和2.3%,以色列 40 ,美国 48 为3.92%(图2)。日本≥40岁成人高度近视患病率为5.7% 49 ,新加坡≥40岁为5.0%,台湾≥65岁为4.2% 50 ,澳大利亚≥49岁为2.7% 51 。
图2:青年人高度近视的患病率。

The prevalence of high myopia in young adults (aged between 18 and 40 years) is low in Denmark46, Australia47, Israel40 and the USA48. By contrast, high prevalence estimates have been reported in South Korea34, Taiwan35 and several major cities in China42,43,44. Limited data are available in other regions such as South America and Africa.
在丹麦 46 、澳大利亚 47 、以色列 40 和美国 48 ,年轻人(年龄在18至40岁之间)的高度近视患病率较低。相比之下,韩国 34 、台湾 35 和中国几个主要城市 42,43,44 报告的流行率估计值较高。南美洲和非洲等其他区域的数据有限。
A generational lag seems to exist for myopia. The incidence of early-onset myopia (school myopia, occurring before the age of 11 years)52 is increasing, leaving more time for progression to high myopia until refraction stabilizes in the mid-20s53,54. The increase in the prevalence of early-onset myopia in individuals who develop high myopia suggests a worsening epidemic over the next few decades as a substantial proportion of these individuals with high myopia will develop pathologic myopia55. These individuals will also be at risk of other ocular comorbidities that lead to low vision with advanced age and increased health-care costs56,57. Estimates for Singapore suggest an extremely high prevalence of myopia by 2050, with 83% of the population (5 million of 6 million) having some form of myopia, 15% of whom (900,000 individuals) will present with high myopia58. Individuals with high myopia have an increased risk of myopia-related complications that can cause blindness, for example, myopic macular degeneration (MMD), which affects 1–4% of adults (3.8% in Singapore59, 3.1% in Beijing, China60, and 0.9% in Handan, China61). However, the differences in the reported prevalence rates between populations may be due to varying definitions of MMD, as the International Photographic Classification and Grading System for Myopic Maculopathy (the Meta Analysis of the Pathologic Myopia, META-PM) was only proposed in 2015 (ref.62). Owing to the increased prevalence of high myopia, MMD rates are expected to increase in the next few years and public health strategies to slow the progression of low myopia to high myopia are important to prevent severe disease and complications associated with pathologic myopia.
近视似乎存在代际滞后。早发性近视(学校近视,发生在11岁之前) 52 的发病率正在增加,为发展为高度近视留下了更多的时间,直到屈光稳定在25岁左右 53,54 。在发展为高度近视的个体中早发性近视患病率的增加表明在未来几十年中流行病将恶化,因为这些高度近视的个体中的相当一部分将发展为病理性近视 55 。这些人还将面临其他眼部共病的风险,这些共病会随着年龄的增长导致视力低下和医疗保健费用增加 56,57 。对新加坡的估计表明,到2050年,近视的患病率极高,83%的人口(600万人中的500万人)患有某种形式的近视,其中15%(900,000人)将出现高度近视 58 。高度近视的个体患近视相关并发症的风险增加,这些并发症可能导致失明,例如近视性黄斑变性(MMD),其影响1-4%的成年人(新加坡为3.8% 59 ,中国北京为3.1% 60 ,中国邯郸为0.9% 61 )。然而,人群间报告患病率的差异可能是由于MMD的不同定义,因为近视黄斑病变的国际摄影分类和分级系统(病理性近视的荟萃分析,META-PM)仅在2015年提出(参考文献。 62 ).由于高度近视患病率的增加,MMD率预计在未来几年将增加,并且减缓低度近视向高度近视发展的公共卫生策略对于预防与病理性近视相关的严重疾病和并发症是重要的。
Mechanisms/pathophysiology
机制/病理生理学
A better understanding on the mechanism and pathophysiology as well as the risk factors plays a central role in the prevention and management of the onset and progression of myopia. Similar to many complex diseases, myopia is attributable to the interaction of genetic and environmental factors that results in excessive axial eye growth.
更好地了解近视的机制和病理生理学以及危险因素在预防和控制近视的发生和发展中起着核心作用。与许多复杂的疾病类似,近视可归因于遗传和环境因素的相互作用,导致眼轴过度生长。
Environmental risk factors
环境风险因素
Education and near-work activities
教育和近距离工作活动
Myopia seems to be strongly associated with educational attainment or educational intensity. In almost all studies, populations with higher levels of education tend to have higher rates of myopia than populations with lower rates of education. For example, a high prevalence of myopia has been reported in populations that receive intensive education at a young age, such as Jewish boys in Israel who received Orthodox or traditional Orthodox education63. By contrast, East Asian populations who receive less intensive education have a low and similar prevalence of myopia to that in most western countries38.
近视似乎与教育程度或教育强度密切相关。在几乎所有的研究中,受教育程度较高的人群比受教育程度较低的人群患近视的几率更高。例如,据报道,在年轻时接受强化教育的人群中,近视患病率很高,如以色列接受东正教或传统东正教教育的犹太男孩 63 。相比之下,接受较少强化教育的东亚人口的近视患病率较低,与大多数西方国家相似 38 。
In addition, the effect of education can be observed in historical changes in myopia prevalence. The prevalence of myopia was only 1–2% in societies with, at most, limited formal education and gradually increased following the introduction of rudimentary education such as in the Inuit population64. Moreover, the rise in myopia prevalence in East and Southeast Asia has paralleled the introduction of mass intensive schooling. One of the best examples is the change in the prevalence of myopia in Chinese mainland, which was lower than in other regions of Southeast Asia but started to increase dramatically to levels similar to those of other Southeast Asian nations after the end of the Cultural Revolution that led to the expansion of education up to tertiary levels2. Well-documented rural and urban differences in China also reflect the effect of educational intensity65. Of note, there is also a general trend for those from higher socioeconomic status (SES) backgrounds to present with higher levels of myopia than those from lower SES backgrounds in addition to a higher prevalence of myopia among those of high SES backgrounds, possibly because of the positive association between higher SES and higher levels of education66.
此外,教育的效果可以在近视患病率的历史变化中观察到。在正规教育最多有限的社会中,近视的患病率仅为1-2%,随着基础教育的引入,近视的患病率逐渐上升,例如在因纽特人中。此外,东亚和东南亚近视患病率的上升与大规模强化学校教育的引入并行。一个最好的例子是中国大陆近视患病率的变化,它低于东南亚其他地区,但在文化大革命结束后开始急剧增加,达到与其他东南亚国家相似的水平,文化大革命导致教育扩展到高等教育 2 。中国有据可查的城乡差异也反映了教育强度 65 的影响。值得注意的是,除了高社会经济地位背景的人近视患病率更高之外,来自较高社会经济地位背景的人比来自较低社会经济地位背景的人近视程度更高,这也是一个普遍趋势,这可能是因为较高社会经济地位背景和较高教育水平之间的正相关 66 。
A link between myopia prevalence and educational level was first speculated by Kepler almost 400 years ago67. Since then, the direction of causation and the mechanisms involved have been debated; education is a proxy for near-work activities but disentangling reading, writing, watching TV, video gaming and screen time is difficult. A meta-analysis confirmed that more time spent on near-work activities was associated with 14% increased odds of myopia and the odds of myopia increase by 2% for every additional dioptre-hour of near-work per week9. Diopter-hour is a surrogate variable, taking into accout both viewing distance and duration, calculated as 3 hours of reading plus 2 hours of computer use plus 2 hours of video game use per day9. It is unclear whether children with a genetic predisposition for myopia gravitate towards academic pursuits or whether a genetic predisposition to spend more years in education causes myopia. However, a Mendelian randomization study showed that genetic variants associated with more years of schooling were statistically associated with a higher severity of myopia but not vice versa, with little evidence to suggest that myopia affected education, which strongly supports a causal role of education on myopia development68.
大约400年前,开普勒首次推测了近视患病率和教育水平之间的联系 67 。从那时起,因果关系的方向和所涉及的机制一直在争论;教育是近距离工作活动的代表,但理清阅读、写作、看电视、视频游戏和屏幕时间是困难的。一项荟萃分析证实,花在近距离工作活动上的时间越多,近视几率增加14%,每周近距离工作每增加一屈光度小时,近视几率增加2% 9 。屈光度小时是一个替代变量,考虑了观看距离和持续时间,计算为每天3小时的阅读加上2小时的电脑使用加上2小时的视频游戏使用 9 。目前还不清楚有近视遗传倾向的儿童是否倾向于学术追求,或者花更多时间接受教育的遗传倾向是否会导致近视。然而,一项孟德尔随机化研究表明,与受教育年限更长相关的基因变异在统计上与近视的严重程度更高相关,但反之亦然,几乎没有证据表明近视影响教育,这有力地支持了教育对近视发展的因果作用 68 。
Outdoor activities 户外活动
In the past decade, the time that children spend outdoors in bright light has been identified as a protective factor for myopia. This effect has been repeatedly, although not universally, reported in both cross-sectional and longitudinal epidemiological studies69,70,71,72. It has also been investigated in school-based randomized controlled trials (RCTs) and even as a nation-wide strategy in Taiwan. Results from a 3-year RCT in Guangzhou, China, suggested that an additional 40 minutes of outdoor time per day reduced myopia incidence by 20%12. The protective effect of more outdoor time was further confirmed in an RCT in Taiwan13. The same investigators in Taiwan reported that the prevalence of myopia was reduced from 49.4% in 2012 to 46.1% in 2015, when an outdoor time intervention programme was implemented73. The association between outdoor light exposure and myopia has been further supported by some observational studies on seasonal variation and myopia development, which found that myopia progression and eye growth were slower in the summer74. The mechanism seems to involve an increased release of dopamine, a neurotransmitter that, in the retina, mediates eye growth stimulated by bright outdoor light75,76. The idea that light intensity influences myopia development has been strongly supported by results from animal studies. Some forms of experimentally induced myopia (for example, form deprivation myopia) can be almost inhibited by exposing the animals to 15,000 Lux laboratory bright lights versus 500 Lux illuminance75. This effect appears to be mediated by dopamine acting on D2-dopamine receptors in most species76.
在过去的十年里,儿童在户外明亮光线下度过的时间被认为是近视的一个保护因素。这种影响在横断面和纵向流行病学研究 69,70,71,72 中被反复报道,尽管不是普遍报道。它还在以学校为基础的随机对照试验(RCT)中进行了研究,甚至在台湾作为一项全国性的战略。在中国广州进行的一项为期3年的RCT的结果表明,每天额外的40分钟户外时间可以降低20%的近视发病率。更多户外时间的保护作用在台湾的RCT 13 得到了进一步证实。台湾的同一调查人员报告称,近视患病率从2012年的49.4%降至2015年的46.1%,当时实施了户外时间干预计划 73 。一些关于季节变化和近视发展的观察性研究进一步支持了户外光照和近视之间的联系,这些研究发现近视进展和眼睛生长在夏季 74 较慢。该机制似乎涉及多巴胺的释放增加,多巴胺是一种神经递质,在视网膜中,介导明亮的室外光线刺激的眼睛生长。光强度影响近视发展的观点得到了动物研究结果的有力支持。某些形式的实验诱导的近视(例如,形觉剥夺性近视)几乎可以通过将动物暴露于15,000勒克斯的实验室强光而不是500勒克斯的照度 75 来抑制。在大多数物种中,这种效应似乎是由作用于D2多巴胺受体的多巴胺介导的 76 。
Some alternative hypotheses, such as increased UV exposure operating via vitamin D levels, offer other potential mechanisms underlying the effect of increased outdoor time on the prevention of myopia77,78. In addition, violet light exposure suppressed myopia progression in both an animal model and in a retrospective study of children who wore violet light-blocking eyeglasses or contact lenses79, suggesting that exposure to short wavelength ambient light may slow myopia progression. Further animal experiments have been performed to understand the interaction between sunlight exposure and myopia in the context of myopic defocus models in outdoor versus indoor settings; however, owing to inconsistencies between studies, further investigations are required75,80,81,82. Whether the wavelength or intensity of light or the duration of light exposure can effectively block myopia development is unknown, but outdoor light exposure does seem to play a role in reducing the level of myopia and its progression.
一些替代假设,如通过维生素D水平增加紫外线暴露,提供了增加户外时间预防近视的其他潜在机制。此外,在动物模型和对佩戴阻挡紫光眼镜或隐形眼镜 79 的儿童的回顾性研究中,紫光暴露抑制了近视进展,这表明暴露于短波长环境光可能会减缓近视进展。已经进行了进一步的动物实验,以了解在室外与室内环境中近视散焦模型的背景下阳光照射和近视之间的相互作用;然而,由于研究之间的不一致,需要进一步的调查 75,80,81,82 。光的波长或强度或光照的持续时间是否能有效阻止近视的发展尚不清楚,但户外光照似乎确实在降低近视的水平及其进展方面发挥了作用。
Genetic factors 遗传因素
A genetic contribution to myopia has been postulated for many years83 and is supported by the increased clustering of myopia cases within families, particularly in the offspring of parents with myopia8 and in those with close relatives who have myopia84. There is also a higher correlation of myopia onset in monozygotic twins than in dizygotic twins85,86,87. Genetic linkage studies have identified more than 20 regions across the genome linked to myopia, indicating that the origin of myopia is multigenic and heterogeneous88. Exome sequencing and whole-genome sequencing have greatly extended findings from linkage studies89. Convincing evidence has emerged that rare, missense or loss-of-function variants in ARR3, BSG, CTSH, CCDC111, LEPREL1, LOXL3, LRPAP1, NDUFAF7, P4HA2, SCO2, SLC39A5, UNC5D and ZNF644 can cause high myopia89. The inheritance pattern of most of these genes is autosomal dominant with the exception of ARR3 (X-linked) and LEPREL1 and LOXL3 (autosomal recessive). These discoveries give insight into the biological mechanisms causing high myopia and also offer the prospect of specific, targeted therapies.
近视的遗传因素已被假设多年 83 ,并得到家庭内近视病例聚集增加的支持,特别是在患有近视 8 的父母的后代和患有近视 84 的近亲中。同卵双胞胎的近视发病相关性也高于异卵双胞胎 85,86,87 。遗传连锁研究已经确定了基因组中与近视相关的20多个区域,表明近视的起源是多基因和异质性的 88 。外显子组测序和全基因组测序极大地扩展了连锁研究的发现 89 。令人信服的证据表明,ARR3、BSG、CTSH、CCDC111、LEPREL1、LOXL3、LRPAP1、NDUFAF7、P4HA2、SCO2、SLC39A5、UNC5D和ZNF644中的罕见、错义或功能缺失变异可导致高度近视 89 。除了ARR3(X连锁)和LEPREL1和LOXL3(常染色体隐性)之外,这些基因的大多数遗传模式是常染色体显性的。这些发现有助于深入了解导致高度近视的生物学机制,也为特定的靶向治疗提供了前景。
The first two large genome-wide association studies (GWAS) for refractive error, which were conducted by the Consortium for Refractive Error and Myopia (CREAM) and 23andMe, identified single-nucleotide polymorphisms (SNPs) at 24 genetic loci for refractive error and at 22 loci for the age of myopia onset in a sample of almost 80,000 individuals90,91. Together, these studies identified 39 loci associated with refractive error and myopia. Of note, a large degree of overlap existed for the loci identified in both studies92, even though the CREAM analysis was based on a complete ophthalmic examination90, whereas the 23andMe study was based on questions of whether participants had ever been diagnosed with near-sightedness and, if so, at what age91. In both of these studies and subsequent GWAS analyses, the most highly risk-conferring SNPs had effects equivalent to a subclinical refractive change of only 0.20 D, indicating that myopia is largely polygenic and may also involve rare variants of large effect size92. In addition, a meta-analysis combining GWAS data from the CREAM and 23andMe studies (amounting to >160,000 individuals) and replicated in an independent cohort of 95,505 individuals from the UK Biobank increased the number of independent signals to 161 loci associated with refractive error and myopia93. Of note, there was a high genetic correlation between European and Asian individuals (>0.78) in these studies, highlighting the genetic similarities in myopia susceptibility between different ethnic populations90. A GWAS meta-analysis published in 2020 included samples from the CREAM consortium, 23andMe, UK Biobank and the Genetic Epidemiology Research on Adult Health and Ageing (GERA) study and identified an additional 336 novel loci in a combined sample of 542,934 individuals94. In total, the identified SNPs that are associated with refractive error explain ~12.1% of the variance of myopia94 with simulation studies suggesting that GWAS of larger sample sizes may be able to increase this figure closer to the 30–35% heritability observed in family studies95. Polygenic risk scores for predicting which children will develop myopia or high myopia by adulthood also show promise; the best-performing models have an area under the receiver operating characteristics curve of 0.67 for myopia and 0.75 for high myopia94,96.
由屈光不正和近视联盟(CREAM)和23andMe进行的前两项大型屈光不正全基因组关联研究(GWAS)在近80,000名个体 90,91 的样本中,在屈光不正的24个基因位点和近视发病年龄的22个基因位点确定了单核苷酸多态性(SNPs)。这些研究总共确定了39个与屈光不正和近视相关的位点。值得注意的是,两项研究 92 中确定的基因座存在很大程度的重叠,尽管CREAM分析是基于完整的眼科检查 90 ,而23andMe研究是基于参与者是否曾被诊断为近视,如果是,在什么年龄 91 的问题。在这两项研究和随后的GWAS分析中,风险最高的SNPs的效应相当于仅0.20 D的亚临床屈光变化,这表明近视在很大程度上是多基因的,也可能涉及大效应大小 92 的罕见变异。此外,一项荟萃分析结合了来自CREAM和23andMe研究的GWAS数据(总计超过160,000人),并在来自英国生物银行的95,505人的独立队列中重复,将与屈光不正和近视 93 相关的独立信号数量增加到161个位点。值得注意的是,在这些研究中,欧洲和亚洲个体之间存在高度的遗传相关性(>0.78),突出了不同种族人群之间近视易感性的遗传相似性 90 。 2020年发表的一项GWAS荟萃分析包括来自CREAM consortium、23andMe、英国生物银行和成人健康和老龄化遗传流行病学研究(GERA)研究的样本,并在542,934名个体 94 的组合样本中确定了另外336个新基因座。总的来说,已鉴定的与屈光不正相关的SNPs解释了约12.1%的近视方差 94 模拟研究表明,较大样本量的GWAS可能能够增加这一数字,更接近家族研究 95 中观察到的30-35%的遗传率。预测哪些儿童成年后会发展成近视或高度近视的多基因风险评分也显示出希望;性能最佳的模型在接收器工作特性曲线下的面积对于近视为0.67,对于高度近视为0.75 94,96 。
Assessment of the 39 SNPs identified in the CREAM and 23andMe studies indicated that some SNPs were associated with different ages of myopia onset. Indeed, three loci (GJD2, CHRNG and ZIC2) were associated with the axial length to corneal radius (AL/CR) ratio in those <10 years of age, whereas four loci (BMP2, KCNQ5, A2BP1 and CACNA1D) were associated with the AL/CR ratio in those 10–25 years of age and a further 20 loci were associated with the AL/CR ratio in adults (>25 years of age)97. These findings provide possible genetic mechanisms related to the degree of myopia severity whereby higher and more pathological forms of myopia have an earlier age of onset.
对CREAM和23andMe研究中鉴定的39个SNPs的评估表明,一些SNPs与不同年龄的近视发病相关。事实上,三个位点(GJD2、CHRNG和ZIC2)与<10岁人群的眼轴长度与角膜半径(AL/CR)比率相关,而四个位点(BMP2、KCNQ5、A2BP1和CACNA1D)与10-25岁人群的AL/CR比率相关,另外20个位点与成人(>25岁)的AL/CR比率相关。这些发现提供了与近视严重程度相关的可能遗传机制,由此,更高和更病理形式的近视具有更早的发病年龄。
Genes associated with myopia risk encode proteins that are involved in the development of every anatomical component of the eye. Several different biological pathways, including neurotransmission (GJD2 and GRIA4), ion transport (KCNQ5), retinoic acid metabolism (RDH5), extracellular matrix remodelling (LAMA2 and BMP2) and eye development (SIX6 and PRSS56), have been implicated, which provides support for a retina to sclera signalling cascade in myopia92. The most recent GWAS also identified unexpected links between myopia susceptibility and specific retinal or corneal dystrophies, anomalies of the crystalline lens, circadian rhythm and pigmentation traits as well as links with Wnt signalling94. A GWAS on ocular traits, including axial length, has identified an additional nine gene loci, of which two (RSPO1 and ZNRF3) are also involved in Wnt signalling, indicating shared genes between ocular traits and myopia98.
与近视风险相关的基因编码蛋白质,这些蛋白质参与眼睛每个解剖成分的发育。涉及几种不同的生物学途径,包括神经传递(GJD2和GRIA4)、离子转运(KCNQ5)、视黄酸代谢(RDH5)、细胞外基质重塑(LAMA2和BMP2)和眼睛发育(SIX6和PRSS56),这为近视 92 中的视网膜至巩膜信号级联提供了支持。最近的GWAS还确定了近视易感性与特定视网膜或角膜营养不良、晶状体异常、昼夜节律和色素沉着特征之间的意外联系,以及与Wnt信号 94 的联系。一项关于眼部特征(包括眼轴长度)的GWAS已经确定了另外九个基因位点,其中两个(RSPO1和ZNRF3)也参与Wnt信号传导,表明眼部特征和近视 98 之间有共同的基因。
Gene–environment interactions
基因——环境相互作用
Many questions regarding the genetic contribution to myopia remain unanswered. The most fundamental of these is the conundrum of consistent evidence for genetic involvement in myopia despite the rapid increase in myopia prevalence over a single generation, particularly in South East Asian nations, which is a much too short time period for changes in the gene pool to have occurred. The most straightforward explanation for this paradox is that genes and the environment act together in causing myopia through gene–environment (G×E) interactions (Fig. 3).
许多关于近视的遗传因素的问题仍然没有答案。其中最基本的难题是,尽管近视患病率在一代人的时间内迅速增加,特别是在东南亚国家,但遗传参与近视的一致证据是一个难题,对于基因库的变化来说,这是一个太短的时间。对这一悖论最直接的解释是,基因和环境通过基因——环境(G × E)相互作用共同导致近视(图3)。
图3:近视中的基因——环境相互作用。

A widely adopted definition of gene–environment interactions (G×E) is that a genetic variant has a different magnitude of association (effect size) with a trait dependent on exposure to a specific environmental factor. In the absence of G×E interactions, an increased genetic risk of myopia and exposure to a high-risk or low-risk environment have independent effects, represented as a parallel relationship between genetic risk and refractive error in each environment (panel a). G×E interactions lead to non-parallel relationships across environments between genetic risk and refractive error (panels b–e). No environmental risk in individuals at low genetic risk (panels b,c). No genetic risk in individuals exposed to the low risk environment (panel d). Genetic predisposition to myopia reverses depending on environmental exposure (panel e). If a sample comprises approximately equal numbers of individuals from the high-risk and low-risk environments, the average effect will lie midway between the effects in each environment (green line) (panels c–e). A genome-wide association study for refractive error that lacks information on environmental exposures will generally be able to detect genetic effects unless the genetic predisposition to myopia reverses in different environments (green lines).
基因——环境相互作用(G × E)的一个广泛采用的定义是,遗传变异与依赖于特定环境因素的性状具有不同程度的关联(效应大小)。在没有G × E相互作用的情况下,近视遗传风险的增加和暴露于高风险或低风险环境具有独立的影响,表现为每个环境中遗传风险和屈光不正之间的平行关系(图A)。G × E相互作用导致遗传风险和屈光不正之间跨环境的非平行关系(图B-E)。低遗传风险个体无环境风险(图b、c)。暴露在低风险环境中的个体没有遗传风险(图d)。近视的遗传易感性根据环境暴露而逆转(图e)。如果样本由来自高风险和低风险环境的大约相同数量的个体组成,平均效应将位于每个环境中效应的中间(绿线)(图C-E)。缺乏环境暴露信息的屈光不正全基因组关联研究通常能够检测到遗传效应,除非近视的遗传易感性在不同环境中逆转(绿线)。
Progress towards the discovery of G×E interactions in myopia and high myopia has lagged far behind that of detecting genetic variants with purely main (non-interaction) effects99. Most research has focused on education or near-work as the environmental risk factor of interest and exposures, such as years of schooling, are routinely collected in large study cohorts. Other factors, such as time spent outdoors, are rarely or inadequately measured, which could explain why no G×E interaction involving time outdoors has yet been discovered100. An early, pioneering study comparing monozygotic to discordant twins demonstrated greater concordance for myopia and reading and/or near-work habits in identical twins than in discordant twins101. Another innovative study reported that the interaction between a child’s number of parents with myopia (zero, one or two) and whether they read fewer or more than two books per week was predictive of the child developing moderate myopia (P = 0.003)102. However, this study102 took no account of ethnicity; hence, the interaction could have been the result of the prevalence of myopia and the average number of books read varying by ethnicity103.
在近视和高度近视中发现G × E相互作用的进展远远落后于检测具有纯主要(非相互作用)效应的遗传变异 99 。大多数研究都集中在教育或近距离工作上,因为感兴趣的环境风险因素和暴露,如受教育年限,通常是在大型研究队列中收集的。其他因素,如花在户外的时间,很少或不充分测量,这可以解释为什么还没有发现涉及户外时间的G × E相互作用 100 。一项早期的开创性研究比较了同卵双胞胎和不和谐双胞胎,表明同卵双胞胎的近视、阅读和/或近距离工作习惯比不和谐双胞胎更一致 101 。另一项创新研究报告称,儿童近视父母的数量(零、一或两个)与他们每周阅读少于或多于两本书之间的相互作用预示着儿童发展为中度近视(P=0.003) 102 。然而,这项研究 102 没有考虑种族;因此,这种相互作用可能是近视流行和平均阅读书籍数量因种族而异的结果 103 。
In comparison with these early studies, work in the past decade has focused on the role of specific genetic variants, which offers a greater opportunity to identify robust, replicable findings. To date, studies investigating the interactions between SNPs and education and/or near-work have implicated the genes MMP2, SHISA6, DNAH9, GJD2, ZMAT4, SFRP1, APLP2, DLX1, BICC1 and A2BP1 (refs100,104,105,106). All except two of these ten genes were initially identified in a GWAS for refractive error and subsequently shown to have G×E effects. Interestingly, for each of the genes reported to have an interaction with education and/or near-work, the effect of the lead genetic variant at the locus was larger in individuals exposed to a higher rather than a lower level of education and/or near-work, consistent with the theory that genetic susceptibility to myopia is mediated, at least in part, through greater susceptibility to environmental risk factors107. Independent replication of G×E effects has been demonstrated for only two of the genes listed above (ZMAT4 and APLP2); thus, these findings need to be interpreted with caution. Other researchers have applied an agnostic approach to detect G×E interacting variants through conditional quantile regression analysis, which tests for gene variants that have larger effects in some individuals than in others. Conditional quantile regression analysis in 146 GWAS variants for refractive error suggested that interaction effects were present in 128 (88%) variants, although whether these were due to G×E or gene–gene interaction effects was unclear108. Laboratory studies of myopia in chicks have also led to the discovery of a novel G×E interaction, which involved the PIK3CG–PRKAR2B locus and the time children spent reading109.
与这些早期研究相比,过去十年的工作集中在特定基因变异的作用上,这为确定稳健、可复制的发现提供了更大的机会。迄今为止,调查SNPs与教育和/或近距离工作之间相互作用的研究涉及基因MMP2、SHISA6、DNAH9、GJD2、ZMAT4、SFRP1、APLP2、DLX1、BICC1和A2BP1(参考文献 100,104,105,106 )。除了两个基因之外,这十个基因中的所有基因最初都在GWAS中被鉴定为屈光不正,随后被证明具有G × E效应。有趣的是,对于报道的与教育和/或近距离工作有相互作用的每个基因,在暴露于较高而非较低教育和/或近距离工作水平的个体中,该基因座的先导遗传变异体的影响更大,这与近视的遗传易感性至少部分通过对环境风险因素的更大易感性介导的理论一致 107 。只有上面列出的两个基因(ZMAT4和APLP2)证明了G × E效应的独立复制;因此,这些发现需要谨慎解读。其他研究人员应用了一种不可知的方法,通过条件分位数回归分析来检测G × E相互作用的变异体,该分析测试在一些个体中比在其他人中具有更大影响的基因变异体。对146个屈光不正GWAS变异体的条件分位数回归分析表明,128个(88%)变异体存在相互作用效应,尽管这些效应是由于G × E还是基因——基因相互作用效应尚不清楚 108 。对小鸡近视的实验室研究也导致了一种新的G × E相互作用的发现,这种相互作用涉及PIK3CG-PRKAR2B基因座和儿童阅读 109 的时间。
Eye growth 眼生长
Children are generally born hyperopic and few individuals are affected by myopia. Emmetropization occurs during the first 2 years of infancy110. This process typically peaks at the end of ~2 years of age when the eye has not become emmetropic but resides at around +1.0–1.5 D — a level of hyperopia in which accommodation can be used to produce good visual acuity111. This change of refraction over time of development involves reductions in corneal112 and crystalline lens power113 as well as an increase in axial length114.
儿童通常天生远视,很少有人受到近视的影响。正视化发生在婴儿期的前2年 110 。这一过程通常在大约2岁时达到高峰,此时眼睛还没有变得正视,而是停留在大约+1.0-1.5 D——这是一种远视水平,在这种水平下,调节可以用来产生良好的视力 111 。随着发育时间的推移,这种屈光变化包括角膜 112 和晶状体度数 113 的减少以及眼轴长度 114 的增加。
After infancy, normal development of the eye leads to an end to changes in corneal power, while crystalline lens power continues to decline and axial length continues to elongate, albeit more slowly, to maintain the emmetropization status. By the time children start primary school, there is generally little development of myopia, although the prevalence of myopia seems to start to rise in preschool years in some parts of East Asia115. Once children enter school, the rate of axial elongation increases while the rate of lens power loss continues to decline116, leading to hyperopic shifts in refraction, counteracted by the myopic shifts in refraction that occur owing to axial elongation116. This balance between axial elongation and loss of lens power is not broken unless myopia develops. Myopic shifts in refraction become predominant, until axial elongation finally becomes minimal at some stage in the third decade of life117. The loss of crystalline lens power continues at a very low rate for most of the adult life, resulting in slow hyperopic shifts in refraction.
婴儿期后,眼睛的正常发育导致角膜光焦度变化的结束,而晶状体光焦度继续下降,眼轴长度继续拉长,尽管更慢,以维持正视化状态。到儿童开始上小学时,近视的发展一般很少,尽管在东亚的一些地区,近视的患病率似乎在学龄前开始上升 115 。一旦儿童进入学校,轴向伸长率增加,而晶状体光焦度损失率继续下降 116 ,导致远视屈光偏移,被由于轴向伸长 116 而发生的近视屈光偏移抵消。除非近视发展,否则轴向伸长和晶状体屈光力损失之间的平衡不会被打破。屈光的近视偏移变得主要,直到轴向伸长最终在生命的第三个十年的某个阶段变得最小 117 。在成人生活的大部分时间里,晶状体屈光力的丧失以非常低的速度持续,导致屈光的缓慢远视偏移。
Regulation of eye growth 眼生长调节
Animal models have been central to our understanding of the aetiology of myopia as many characteristic features of human myopia occur in animals, including an axially elongated eye, retinal and scleral thinning, and relative stability of refractive error beyond the critical period of juvenile development. Several animal models, including chicks, tree shrews, marmosets, monkeys, guinea pigs, mice and fish, have been used to experimentally induce myopia through lens-induced myopia and form-deprivation myopia and have provided important information on the potential pathways and development in a controlled laboratory manner to minimize heterogeneous effects118.
动物模型是我们理解近视病因学的核心,因为人类近视的许多特征发生在动物身上,包括轴向拉长的眼睛、视网膜和巩膜变薄以及屈光不正超过青少年发育关键期的相对稳定性。包括小鸡、树鼩、狨猴、猴子、豚鼠、小鼠和鱼在内的几种动物模型已被用于通过晶状体诱导的近视和形觉剥夺性近视实验性诱导近视,并以受控的实验室方式提供了关于潜在途径和发展的重要信息,以最小化 118 的异质性效应。
Early studies demonstrated that modest changes to the sharpness of the visual image received by the eye during a critical period of development, such as that produced by form deprivation, resulted in severe axial myopia in almost all species examined118. Further studies in which innate refractive errors were simulated by raising animals wearing a spectacle lens in front of one or both eyes (known as lens-compensation strategies) have provided the most clinically relevant insights into the effects of vision on refractive development119,120. In particular, these experiments demonstrated that altering the eye’s refractive status with a negative-powered or positive-powered lens can produce predictable changes in refractive development (that is, the eye can detect the presence of the induced refractive error and grow in a manner to eliminate the error). These compensating changes in refractive development reflect alterations in the eye’s elongation rate through the upregulation or downregulation of the rate of vitreous chamber elongation (emmetropization) and demonstrate a visually guided feedback process until the eye has ‘grown into focus’. Qualitatively similar results have been obtained in many different species118,121, demonstrating that the vision-dependent mechanisms regulating refractive development are fundamental from an evolutionary perspective. These vision-dependent mechanisms in response to environmental factors are thought to also be responsible for the most common forms of myopia in children.
早期的研究表明,在发育的关键时期,眼睛接收到的视觉图像清晰度的适度变化,如由形式剥夺产生的变化,导致几乎所有被检查的物种都出现严重的轴性近视。在进一步的研究中,通过在一只或两只眼睛前饲养佩戴眼镜片的动物来模拟先天屈光不正(称为晶状体补偿策略),为视觉对屈光发育的影响提供了最具临床相关性的见解 119,120 。特别是,这些实验证明,用负光焦度或正光焦度透镜改变眼睛的屈光状态可以在屈光发育中产生可预测的变化(即,眼睛可以检测到诱导的屈光不正的存在,并以消除该误差的方式生长)。屈光发育中的这些补偿性变化通过上调或下调玻璃体腔伸长率(正视化)反映了眼睛伸长率的变化,并展示了视觉引导的反馈过程,直到眼睛“变得聚焦”。在许多不同的物种 118,121 中获得了定性相似的结果,表明从进化的角度来看,调节屈光发育的视觉依赖机制是基本的。这些视觉依赖机制对环境因素的反应被认为也是儿童最常见形式近视的原因。
In this respect, studies from animal models have provided several insights: hyperopic defocus increases the rate of axial elongation, whereas myopic defocus decreases the rate of axial elongation119; visual signals from the retinal periphery, primarily as a result of areal summation, can dominate central refractive development, irrespective of central visual experience82; when the eye receives competing defocus signals (for example, hyperopic versus myopic defocus), either simultaneously122 or successively123, the more myopic signal dominates eye growth; the effectiveness of optical defocus in altering axial elongation is dependent on the extent of the retina that is defocused124. The influence of these mechanisms is most obvious early in life, but these mechanisms remain active into adulthood and are important for maintaining the eye’s refractive state and the normal balance between the two eyes. As a consequence, environmental stimuli can potentially produce adult-onset and adult progression of myopia125; however, the resulting changes are generally smaller and take longer to develop than those in children126.
在这方面,来自动物模型的研究提供了几个见解:远视散焦增加了轴向伸长率,而近视散焦降低了轴向伸长率 119 ;来自视网膜外围的视觉信号,主要是作为区域总和的结果,可以支配中心屈光发育,而不考虑中心视觉体验 82 ;当眼睛同时 122 或连续 123 接收竞争散焦信号(例如,远视与近视散焦)时,更近视的信号支配眼睛生长;光学散焦在改变轴向伸长方面的有效性取决于在4#时散焦的视网膜范围。这些机制的影响在生命早期最为明显,但这些机制在成年后仍保持活跃,对于维持眼睛的屈光状态和双眼之间的正常平衡非常重要。因此,环境刺激可能会导致成人发病和成人近视进展 125 ;然而,由此产生的变化通常比儿童 126 的变化更小,需要更长的时间来发展。
Mechanisms of eye growth
眼生长机制
Animal models have also demonstrated that growth-regulating mechanisms are located entirely within the eye and continue to function even when the neural eye–brain links are disrupted120. Moreover, eye elongation is regulated by multiple mechanisms across the retina, which operate independently in a regionally selective manner and can produce localized changes in the shape of the posterior globe, probably to optimize the focus of the eye across the visual field126. The growth-regulating cascade has a retina-to-sclera direction beginning in the neural retina and passing through the retinal pigment epithelium (RPE) and choroid to modulate the biochemical and mechanical nature of the sclera, thereby promoting eye length changes that normally eliminate refractive errors120 (Fig. 4). In many respects, this is an intriguing process because, during the first few years of life, this cascade is very successful in achieving a precise balance between the eye’s focal length and its axial length in the majority of individuals despite the fact that the eye is a very fragile tissue that is potentially influenced by multiple factors — a mismatch between the eye’s focal length and axial length that exceeds the thickness of an eyelash is sufficient to produce a detectable alteration in vision. Photoreceptors and contrast-sensitive inner retinal neurons are thought to be early components in the cascade sensing optical errors and initiating signals to increase or decrease axial elongation, apparently through different independent molecular mechanisms127,128. It is not known exactly how the eye determines whether it is far-sighted or near-sighted. However, some studies suggest that the retina can decode the sign of defocus using spectral cues associated with different wavelengths of light129. This may be why alterations in the spectral composition of ambient lighting130,131, genetic alterations in cone photopigment opsins132, and variations in the relative number of middle-wavelength-sensitive and long-wavelength-sensitive cones can influence refractive development.
动物模型还表明,生长调节机制完全位于眼睛内,即使在神经眼脑连接被破坏时也能继续发挥作用。此外,眼睛伸长由视网膜上的多种机制调节,这些机制以区域选择性的方式独立操作,并可以产生后眼球形状的局部变化,可能是为了优化眼睛在整个视野中的焦点 126 。生长调节级联具有从神经视网膜开始并穿过视网膜色素上皮(RPE)和脉络膜的视网膜到巩膜的方向,以调节巩膜的生物化学和机械性质,从而促进通常消除屈光不正 120 的眼长变化(图4)。在许多方面,这是一个有趣的过程,因为在生命的最初几年,这种级联反应非常成功地实现了大多数人眼睛焦距和轴向长度之间的精确平衡,尽管眼睛是一种非常脆弱的组织,可能会受到多种因素的影响——眼睛焦距和轴向长度之间的不匹配超过睫毛的厚度足以产生可检测的视力变化。光感受器和对比敏感的视网膜内层神经元被认为是级联感知光学误差和启动信号以增加或减少轴向伸长的早期成分,显然是通过不同的独立分子机制 127,128 。目前还不知道眼睛是如何判断自己是远视还是近视的。 然而,一些研究表明,视网膜可以使用与不同波长的光 129 相关的光谱线索来解码散焦的迹象。这可能是为什么环境照明 130,131 的光谱组成的改变、视锥光色素视蛋白 132 的遗传改变以及中波长敏感和长波长敏感视锥相对数量的变化会影响屈光发育。
图4:灵长类动物眼睛的磁共振图像,将视觉诱导的近视与对照眼睛生长进行比较。

MRI scans of a control (panel a) and treated eye (panel b) of a monkey with a high-degree of monocular, vision-induced myopia. The outlines of the control eye (red trace) and treated eye (blue trace) are superimposed after rotating the control eye image around the optic axis so that the nasal (N) retinas (the part of the retina closest to the nose) are shown to the right for both eyes and temporal (T) (retinal part nearest the temple of the head) are shown to the left (panel c). The superimposed images demonstrated that the myopia reflects an increase in vitreous chamber depth whereas the cornea, anterior chamber and crystalline lens are largely unaffected. Several components of the eye adapt to the effects of vision on refractive development (panel d). Defocus is the optimal stimulus for eye growth and changes in the eye’s effective focus can influence a variety of neuromodulators and signal molecules that influence refractive development and are likely to be linked to myopia. RPE, retinal pigment epithelium; VIP, vasoactive intestinal peptide. Adapted with permission from ref.309, Smith, E. L. III Prentice award lecture 2010: a case for peripheral optical treatment strategies for myopia. Optometry Vis. Sci. 88(9). 1029–1044 (https://journals.lww.com/optvissci/pages/default.aspx).
患有高度单眼视觉诱发近视的猴子的对照眼(图A)和治疗眼(图b)的MRI扫描。在围绕视轴旋转控制眼图像之后,叠加控制眼(红色轨迹)和治疗眼(蓝色轨迹)的轮廓,使得对于两只眼睛,鼻(N)视网膜(最靠近鼻子的视网膜部分)显示在右侧,颞(T)(最靠近头部太阳穴的视网膜部分)显示在左侧(图c)。叠加图像显示,近视反映了玻璃体腔深度的增加,而角膜、前房和晶状体基本不受影响。眼睛的几个组成部分适应视觉对屈光发育的影响(图d)。散焦是眼睛生长的最佳刺激,眼睛有效焦点的变化可以影响多种神经调质和信号分子,这些神经调质和信号分子影响屈光发育,并可能与近视有关。RPE,视网膜色素上皮;血管活性肠肽。经参考文献许可改编。 309 ,Smith,E.L.III Prentice Award讲座2010:近视周边光学治疗策略案例。验光视觉。Sci.88(9).1029-1044(https://journals.lww.com/optvissci/pages/default.aspx)。
Within the retina, multiple neural channels, neurochemicals and their receptors have been implicated in the cascade. For instance, selective interruptions and/or adaptations of the ON and OFF retinal channels, which originate at the synapses between photoreceptors and bipolar cells, can have qualitatively different effects on ocular growth and refractive development133,134,135,136,137,138. The exact nature of these pathways is not well understood but several components have been implicated, including retinal dopaminergic mechanisms. In particular, retinal dopamine levels are influenced by various visual stimuli that have been shown to alter eye growth and refractive development and dopamine drugs can alter the course of experimentally induced myopia76. Interestingly, the retinal ON-pathway seems to be a primary driver of retinal dopamine release139. The role of the RPE is probably multifactorial: the RPE has receptors for retinal molecules that have been associated with growth regulation and these can synthesize and release growth factors and cytokines that have been implicated in growth regulation (such as IGF1, TGFβ, FGF, VEGF and BMP)140,141. Thus, the RPE can relay and/or amplify retinal growth signals. In addition, the RPE regulates ion and fluid exchange between the retina and choroid, which probably plays a role in the vision-dependent changes observed in choroidal thickness.
在视网膜内,多个神经通道、神经化学物质及其受体与级联反应有关。例如,起源于光感受器和双极细胞之间突触的开和关视网膜通道的选择性中断和/或适应可以对眼睛生长和屈光发育产生定性不同的影响。这些途径的确切性质还不清楚,但已经涉及到几个组成部分,包括视网膜多巴胺能机制。特别是,视网膜多巴胺水平受到各种视觉刺激的影响,这些视觉刺激已被证明会改变眼睛生长和屈光发育,并且多巴胺药物可以改变实验诱导的近视的进程 76 。有趣的是,视网膜通路似乎是视网膜多巴胺释放的主要驱动力 139 。RPE的作用可能是多因素的:RPE具有与生长调节相关的视网膜分子受体,这些受体可以合成和释放与生长调节相关的生长因子和细胞因子(如IGF1、TGF β、FGF、VEGF和BMP) 140,141 。因此,RPE可以中继和/或放大视网膜生长信号。此外,RPE调节视网膜和脉络膜之间的离子和液体交换,这可能在观察到的脉络膜厚度的视觉依赖性变化中起作用。
The choroid is also a key component. Visual signals that influence refractive development produce changes in choroidal thickness that are in the appropriate direction to reduce optical errors142. In addition, these visual signals modulate, in a bidirectional manner, the synthesis of all-trans-retinoic acid143, a growth factor that modulates scleral proteoglycan synthesis, one of the main structural components of the sclera143,144. The sclera, the connective tissue that defines the eye’s size and shape, represents the final common pathway where visually derived signals produce direction-specific effects. For example, visual stimuli that produce myopia decrease collagen synthesis and increase the synthesis of enzymes that degrade the scleral extracellular matrix, resulting in a thinning of the sclera and altering its biomechanical properties, which makes it more susceptible to stretching and increasing axial elongation145,146,147.
脉络膜也是一个关键的组成部分。影响屈光发育的视觉信号产生脉络膜厚度在适当方向上的变化,以减少光学误差 142 。此外,这些视觉信号以双向方式调节全反式视黄酸 143 的合成,全反式视黄酸 143 是一种调节巩膜蛋白聚糖合成的生长因子,巩膜蛋白聚糖是巩膜 143,144 的主要结构成分之一。巩膜是定义眼睛大小和形状的结缔组织,代表了视觉信号产生方向特异性效应的最终共同途径。例如,产生近视的视觉刺激会减少胶原蛋白的合成,增加降解巩膜细胞外基质的酶的合成,导致巩膜变薄并改变其生物力学特性,这使其更容易受到拉伸并增加轴向伸长 145,146,147 。
Scleral involvement in myopia
近视中的巩膜受累
Typical thinning of the sclera occurs in myopic eyes owing to extracellular matrix (ECM) remodelling, which results in a decline in scleral strength and is accompanied by ocular axial elongation in animal models148,149. The initiators and signalling pathways underlying these events in myopia are largely unknown but single-cell RNA sequencing indicates that hypoxia-inducible factor 1α (HIF1α) signalling can promote myopia through myofibroblast trans-differentiation and a subsequent decrease in collagen content150 in different experimental myopia models. Hence, hypoxia has been suggested to act as a key modulator for scleral ECM remodelling during myopia development. Scleral hypoxia results from a decline in blood perfusion in the choroid. In two guinea pig models of myopia, both choroidal thickness and choroidal blood perfusion were significantly decreased151. It is hypothesized that the visual signal input perceived by the retina is transduced through modulating cell signalling pathway cascades, such as dopamine signalling, which control choroidal blood perfusion and the scleral oxygenation microenvironment. Accordingly, a decline in oxygenation may trigger other downstream events that modulate scleral and ECM integrity, resulting in scleral thinning and myopia induction.
由于细胞外基质(ECM)重塑,近视眼睛中发生典型的巩膜变薄,这导致巩膜强度下降,并在动物模型 148,149 中伴随着眼轴伸长。近视中这些事件背后的起始物和信号通路在很大程度上是未知的,但单细胞RNA测序表明,缺氧诱导因子1 α(HIF1 α)信号可以通过肌成纤维细胞转分化和随后在不同的实验性近视模型中胶原含量 150 的降低来促进近视。因此,缺氧被认为是近视发展过程中巩膜ECM重塑的关键调节剂。巩膜缺氧是由脉络膜血液灌注下降引起的。在两个近视豚鼠模型中,脉络膜厚度和脉络膜血液灌注在2#时均显著降低。假设由视网膜感知的视觉信号输入是通过调节细胞信号通路级联来转导的,例如控制脉络膜血液灌注和巩膜氧合微环境的多巴胺信号。因此,氧合的下降可能触发调节巩膜和ECM完整性的其他下游事件,导致巩膜变薄和近视诱导。
In humans, dramatic reductions in choroidal thickness and choroidal blood perfusion have been observed in highly myopic eyes152,153, which might cause scleral hypoxia, ECM remodelling and myopia development. This would suggest that the hypoxic microenvironment in sclera may be one of the master regulators triggering signal mechanisms in scleral ECM remodelling and myopia development in both experimental animal models and humans. Further support for this mechanism comes from protein–protein network analysis in which a substantial number of interactions were identified between genes in the HIF1α pathway and risk genes of myopia (45 of 145 genes, 31%) and pathologic myopia (10 of 27 genes, 37%) that had previously been identified in GWAS150. Therefore, these findings strongly implicate the involvement of scleral hypoxia as part of the process of human myopia development, although the visual stimulus and its signalling pathway from photoreceptor to sclera and the role of choroidal blood flow require further investigation.
在人类中,在高度近视的眼睛 152,153 中观察到脉络膜厚度和脉络膜血液灌注的显著减少,这可能导致巩膜缺氧、ECM重塑和近视发展。这表明,在实验动物模型和人类中,巩膜中的低氧微环境可能是触发巩膜ECM重塑和近视发展的信号机制的主要调节因子之一。对这一机制的进一步支持来自蛋白质——蛋白质网络分析,其中在HIF1 α途径中的基因与近视(145个基因中的45个,31%)和病理性近视(27个基因中的10个,37%)的风险基因之间确定了大量的相互作用,这些基因以前在GWAS 150 中被确定。因此,这些发现强烈暗示巩膜缺氧是人类近视发展过程的一部分,尽管视觉刺激及其从光感受器到巩膜的信号通路以及脉络膜血流的作用需要进一步研究。
Diagnosis, screening and prevention
诊断、筛查和预防
Visual acuity testing 视力测试
Myopia is characterized as blurred distance vision while near vision remains normal. Standard charts are commonly used to assess distance and near visual acuity. Visual acuity is measured by asking people to discriminate letters of known size, represented as the smallest letter resolved at a given distance and at high contrast. ETDRS charts are the most commonly used charts for both research and clinical practice and use letters with equal recognition difficulty and the log of the minimal angle of resolution (logMAR) principle154. This chart has substantial advantages over the Snellen-type chart, including an equal number of letters per row, equal logarithmic decrement between successive rows and the use of letters that are of more legibility. Visual acuity is often recorded as a fraction, such as a 6-metre notation of 6/12, where 6 indicates that a person needs to be at a distance of 6 meters to be able to see what a person with normal vision would see from a distance of 12 meters. This is equivalent to 20/40 in feet (imperial measure) notation or 0.50 in decimal notation. Normal distance visual acuity would be 6/6 in meters or 20/20 in feet or better, although some preschool children aged 3–6 years may not reach this level of visual acuity155 owing to the immaturity of their visual and cortical processing system156. A greater degree of myopia usually has a greater effect on distance visual acuity, but its influence can vary and often depends on the presence of astigmatism and other factors.
近视的特征是远视模糊,而近视保持正常。标准图表通常用于评估远视和近视敏度。视觉敏锐度是通过要求人们辨别已知大小的字母来测量的,这些字母表示为在给定距离和高对比度下分辨的最小字母。ETDRS图表是研究和临床实践中最常用的图表,使用具有同等识别难度的字母和最小分辨角对数(logMAR)原理 154 。与Snellen型图表相比,这种图表有很大的优势,包括每行字母数相等,连续行之间的对数减量相等,以及使用更易读的字母。视敏度通常被记录为一个分数,例如6/12的6米符号,其中6表示一个人需要在6米的距离才能看到一个视力正常的人在12米的距离看到的东西。这相当于20/40英尺(英制)记数法或0.50十进制记数法。正常的远距离视敏度应该是6/6米或20/20英尺或更好,尽管一些3-6岁的学龄前儿童可能达不到这个视敏度水平 155 ,因为他们的视觉和皮层处理系统 156 不成熟。较大程度的近视通常对远距离视力有较大的影响,但其影响可以变化,并且通常取决于散光和其他因素的存在。
Refraction and ocular examination
屈光和眼部检查
In optometry, refraction is a clinical procedure to measure the ocular refractive status in units of dioptre. Two methods are commonly used to assess the eye’s refractive error. Retinoscopy is a subjective method that requires a technically trained examiner to use a handheld instrument called retinoscope to project a beam of light into the eye and then to observe the reflection from the patient’s retina. When the examiner moves the streak of light across the pupil, by observing the relative movement of the reflection and a lens manually placed in front of the eyes to neutralize the reflection, the examiner estimates the diopter of refractive error. Refraction can also be measured by autorefraction, an objective measurement using a device called an autorefractor. Refraction should be assessed following the pharmacological induction of cycloplegia to prevent the lens of the eye changing focus (accommodation), thereby overestimating the degree of myopia. Atropine, cyclopentolate and tropicamide are the most commonly used cycloplegic agents in children and adolescents. Cycloplegic refraction in children and adolescents is an established clinical consensus, but one study proposed that cycloplegia should also be induced in adults up to 50 years of age because non-cycloplegic refraction can substantially overestimate the prevalence of myopia even in adults157. Complete cycloplegia is achieved when the pupil is dilated to >6 mm and/or a light reflex is absent. Following cycloplegia, retinoscopy or an autorefractor can be used to measure refraction, which should ideally take place in a semi-dark room.
在验光中,屈光是以屈光度为单位测量眼睛屈光状态的临床程序。两种方法通常用于评估眼睛的屈光不正。视网膜镜检查是一种主观方法,需要受过技术训练的检查者使用称为视网膜镜的手持仪器将光束投射到眼睛中,然后观察患者视网膜的反射。当检查者通过观察反射和手动放置在眼睛前面以中和反射的透镜的相对运动来移动光线穿过瞳孔时,检查者估计屈光不正的屈光度。屈光也可以通过自动折射来测量,这是一种使用称为自动折射仪的设备进行的客观测量。应在药物诱导睫状肌麻痹后评估屈光,以防止眼睛的晶状体改变焦点(调节),从而高估近视的程度。阿托品、环喷托酯和托吡卡胺是儿童和青少年最常用的睫状肌麻痹药物。儿童和青少年的睫状肌麻痹性屈光是公认的临床共识,但一项研究提出,50岁以下的成人也应诱发睫状肌麻痹,因为非睫状肌麻痹性屈光可能大大高估近视的患病率,即使在成人 157 中也是如此。当瞳孔放大到>6 mm和/或没有光反射时,就达到了完全的睫状肌麻痹。睫状肌麻痹后,视网膜检影或自动验光仪可用于测量屈光,理想情况下应在半暗的房间内进行。
Myopia is commonly defined as a SE of ≤−0.50 D (refs158,159). In some clinical studies, the SE cut-off value varied from −0.12 D to −1.00 D (refs90,160,161,162,163). The severity of myopia is often categorized as mild (−0.50 D to −3.00 D), moderate (−3.00 D to −5.00 D or −6.00 D) or high (≤−5.00 or −6.00 D) in clinical practice. The threshold for high myopia is an arbitrary clinical definition with little evidence suggesting the sudden development of dramatic pathological retinal changes at either of these threshold points51,60,61.
近视通常定义为≤0.50 D的阿瑟(参考文献 158,159 )。在一些临床研究中,SE临界值从0.12 D到1.00 D不等(参考文献 90,160,161,162,163 )。在临床实践中,近视的严重程度通常分为轻度(-0.50 D至-3.00 D)、中度(-3.00 D至-5.00 D或-6.00 D)或高度(≤-5.00 D或-6.00 D)。高度近视的阈值是一个任意的临床定义,几乎没有证据表明在这些阈值点 51,60,61 的任一处突然出现显著的病理性视网膜变化。
Axial length measurement is a useful examination to monitor the progression of myopia and its effect on ocular shape, but it is not routinely performed in optometry services. It can be obtained using A-scan ultrasonography, B-scan ultrasonography, partial coherence interferometry technology or optical low-coherence reflectometry. In general, optical methods are more accurate than ultrasonographic ones164,165. An axial length >26–27 mm is considered an excessive elongation as pathological signs in the fundus are greatly increased beyond this length166,167 (Fig. 5). An increasing level of refraction is also associated with an increased risk of pathological changes but not all highly myopic eyes develop pathological changes.
眼轴长度测量是监测近视进展及其对眼形影响的有用检查,但在验光服务中不常规进行。它可以使用A扫描超声检查、B扫描超声检查、部分相干干涉测量技术或光学低相干反射术来获得。一般来说,光学方法比超声方法更准确 164,165 。轴向长度>26-27 mm被认为是过度伸长,因为眼底的病理体征在超过该长度 166,167 时会大大增加(图5)。屈光水平的增加也与病理变化的风险增加有关,但并不是所有高度近视的眼睛都会发生病理变化。
图5:病理性近视的视网膜变化。

Pathologic myopia is common in individuals with high myopia and excessive axial elongation. It is characterized by ocular shape changes such as staphyloma and severe forms of myopic maculopathy. Features of pathologic myopia include lesions in the macula, in or around the optic nerve, and in the sclera, including tessellated fundus (panel a), diffuse chorioretinal atrophy (panel b), patchy chorioretinal atrophy (black arrow; panel c), macular atrophy (black arrow; panel d), and lacquer crack (white arrow) and macular haemorrhage (black arrow; panel e).
病理性近视常见于高度近视和眼轴过度伸长的个体。其特征为眼部形状改变,如葡萄肿和严重形式的近视黄斑病变。病理性近视的特征包括黄斑、视神经内或视神经周围以及巩膜中的损伤,包括镶嵌状眼底(图A)、弥漫性脉络膜视网膜萎缩(图b)、斑片状脉络膜视网膜萎缩(黑色箭头;图c)、黄斑萎缩(黑色箭头;图d),以及漆裂(白色箭头)和黄斑出血(黑色箭头;面板e)。
Fundoscopic examination 眼底镜检查
A careful examination of the fundus with a magnified slit lamp non-contact lens or indirect ophthalmoscopy should be performed to confirm and assess myopic pathologies in patients with high myopia, including the existence of diffuse, patchy and macular atrophy (Fig. 5). Of note, assessing peripheral lesions and identifying the margin of a posterior staphyloma can be better observed with wide-field optical coherence tomography (OCT) or 3D MRI than with conventional fundus ophthalmoscopy. Digital fundus imaging under cycloplegia is normally used to record and monitor fundus lesions over time. Fundus photography may fail to detect occult lesions or subtle damage, such as choroidal neovascularization, and the detection of these pathologies may require fundus fluorescein angiography, indocyanine green angiography or OCT. A 3D MRI scan can be used to visualize the entire eye shape in patients with staphylomas168,169, and ultra-wide-field OCT can be used to routinely analyse the shape of the posterior segment and the relationship between the staphyloma and its blinding complications170,171.
应使用放大裂隙灯非接触镜或间接检眼镜仔细检查眼底,以确认和评估高度近视患者的近视病理,包括弥漫性、斑片状和黄斑萎缩的存在(图5)。值得注意的是,与传统的眼底眼底镜检查相比,宽视野光学相干断层扫描(OCT)或3D MRI可以更好地观察周围病变和识别后部葡萄肿的边缘。睫状肌麻痹下的数字眼底成像通常用于记录和监测随时间推移的眼底病变。眼底摄影可能无法检测隐匿性病变或细微损伤,如脉络膜新生血管,这些病理的检测可能需要眼底荧光素血管造影、吲哚青绿血管造影或OCT。3D MRI扫描可用于可视化葡萄肿患者的整个眼睛形状 168,169 ,超宽视野OCT可用于常规分析后段的形状以及葡萄肿与其致盲并发症之间的关系 170,171 。
Pathologic myopia 病理性近视
Pathologic myopia is a major cause of decreases in best-corrected visual acuity, especially in east Asia172. A meta-analysis of the pathologic myopia (META-PM) system was proposed by a panel of researchers in which myopic maculopathy is classified into five categories: no myopic retinal lesions (category 0), tessellated fundus only (category 1), diffuse chorioretinal atrophy (category 2), patchy chorioretinal atrophy (category 3) and macular atrophy (category 4) in combination with the three ‘plus signs’ of lacquer crack, myopic choroidal neovascularization and the Fuchs spot. Pathologic myopia has now been defined as myopic maculopathy (META-PM criteria: category 2 or above) or the presence of ‘plus signs’ or posterior staphyloma62,173,174 (Fig. 5). Based on these definitions, accurate examination on the fundus is necessary for the disease staging classification but diagnosis is mainly based on fundus photography, the interpretation of which is subjective. Advances in ocular imaging, such as OCT, enable the accurate diagnosis of each lesion of myopic maculopathy. Diffuse atrophy has been shown to represent an extreme thinning (almost disappearance) of the choroid175,176. Posterior staphyloma is also a fundamental feature of pathologic myopia and is the cause of myopic maculopathy owing to mechanical expansion of the posterior fundus.
病理性近视是最佳矫正视力下降的主要原因,尤其是在东亚 172 。一组研究人员提出了病理性近视(META-PM)系统的荟萃分析,其中近视性黄斑病变分为五类:无近视性视网膜病变(0类)、仅镶嵌眼底(1类)、弥漫性脉络膜视网膜萎缩(2类)、斑片状脉络膜视网膜萎缩(3类)和黄斑萎缩(4类),并伴有漆裂、近视性脉络膜新生血管和Fuchs斑三个“加号”。病理性近视现在被定义为近视性黄斑病变(META-PM标准:2类或以上)或存在“加号”或后部葡萄肿 62,173,174 (图5)。基于这些定义,对眼底的准确检查对于疾病分期分类是必要的,但是诊断主要基于眼底照相,其解释是主观的。眼部成像的进步,如OCT,使得能够准确诊断近视黄斑病变的每个病变。弥漫性萎缩已被证明代表脉络膜极度变薄(几乎消失) 175,176 。后葡萄肿也是病理性近视的基本特征,并且是由于后眼底的机械扩张而导致近视性黄斑病变的原因。
School-based screening 校本筛查
Earlier onset of myopia increases the risk of high myopia later in life, thereby increasing the risk of blindness. Thus, school-based myopia screening could enable the early identification of children with myopia for the effective control of myopia progression.
近视发病较早会增加晚年患高度近视的风险,从而增加失明的风险。因此,以学校为基础的近视筛查可以使近视儿童的早期识别成为可能,从而有效控制近视的发展。
The uncorrected visual acuity (UCVA) test is the most widely used school-based vision screening test. It requires only a visual acuity chart (most commonly a LogMAR chart), adequate illumination and trained nurses, teachers or technicians177,178,179,180. When UCVA is combined with non-cycloplegic autorefraction in serial order, a higher sensitivity is achieved than with either of the two tests alone (63.55%, 78.50% and 84.35%, respectively, for UCVA, non-cycloplegic autorefraction and the combination test)181. However, autorefractometers are not available in most school-based vision screening programmes. In children, vision screening using LogMAR acuity testing can reliably detect myopia (97.8% sensitivity and 97.1% specificity)182,183 but not hyperopia or astigmatism184. In preschool-age children (aged 3–5 years), a UCVA of 6/8 (Snellen equivalent 0.75) or 6/7 (Snellen equivalent 0.85) are considered the best criteria for referral to treatment for ages ≤4 years and ≥5 years, respectively185. In school-age children (aged 6–12 years), the UCVA threshold for referral is 6/7.3 to 6/9.5 (refs182,184). The data from screening and referral results should be tracked in a database to enable the monitoring of changes in myopia prevalence and incidence.
裸眼视力(UCVA)测试是最广泛使用的基于学校的视力筛查测试。它只需要一个视敏度图(最常见的是LogMAR图),足够的照明和训练有素的护士,教师或技术人员 177,178,179,180 。当UCVA与非睫状肌麻痹性自动验光按顺序联合使用时,比单独使用两种测试中的任何一种都具有更高的灵敏度(UCVA、非睫状肌麻痹性自动验光和联合测试分别为63.55%、78.50%和84.35%) 181 。然而,在大多数以学校为基础的视力筛查项目中,自动验光仪是不可用的。在儿童中,使用LogMAR视敏度测试的视力筛查可以可靠地检测近视(97.8%的灵敏度和97.1%的特异性) 182,183 ,但不能检测远视或散光 184 。在学龄前儿童(3-5岁)中,UCVA分别为6/8(Snellen当量0.75)或6/7(Snellen当量0.85)被认为是年龄≤4岁和≥5岁的儿童转诊治疗的最佳标准。在学龄儿童(6-12岁)中,UCVA转诊门槛为6/7.3至6/9.5(参考文献 182,184 )。来自筛查和转诊结果的数据应在数据库中进行跟踪,以便能够监测近视患病率和发病率的变化。
Prevention 预防
Outdoor activity is the main protective factor against myopia69,186. In some areas, schoolchildren spend at least half of their daytime in schools. Accordingly, enhancing outdoor activity programmes or implementing policies for outdoor activities in schools may be highly effective for myopia prevention. Indeed, one of the first school-based myopia prevention programmes, known as Recess Outside Classroom (ROC) in Kaohsiung, Taiwan, required children to leave their classrooms during recess, resulting in an additional 80 minutes of daily time outdoors187. The programme resulted in a 53% reduction in incident myopia after 1 year compared with the control school without ROC intervention. In the cluster randomized Guangzhou Outdoor Activity Longitudinal Trial (GOAL), an additional 40 minutes of outdoor time was added at the end of the school day and resulted in a 23% reduction in incident myopia over 3 years compared with control schools12. The findings of the ROC and GOAL studies seem to show that a dose–response tendency exists between outdoor exposure and a reduction in myopia incidence. Another cluster randomized trial with a school-based outdoor promotion programme effectively reduced myopia progression in both children with or without myopia even in moderate light intensities such as in hallways or under a tree13. Nevertheless, a campaign conducted in Taiwan to educate parents about the benefits of spending time outdoors outside of school time and an incentive-based outdoor programme with family did not have a significant effect on increasing outdoor time12,188. Of note, a 15-year study in Taiwan (the Tian-Tian 120 programme) encouraged schools to allow students to spend 2 hours outdoors daily and demonstrated a reversal in the long-term trend of increased prevalence of reduced visual acuity (which has a high correlation with myopia) in schoolchildren73. This finding shows that a school policy for increasing outdoor time might be a direct and effective way of maintaining visual acuity. The promotion of increased time outdoors for up to 2–3 hours per day is recommended. This recommendation has been adopted in Singapore’s myopia prevention strategy and the Chinese mainland’s myopia prevention plan189.
户外活动是预防近视的主要保护因素 69,186 。在一些地区,学童白天至少有一半时间在学校度过。因此,加强户外活动计划或在学校实施户外活动政策可能对预防近视非常有效。事实上,台湾高雄第一个以学校为基础的近视预防计划之一,即所谓的课外课间休息(ROC),要求孩子们在课间休息时离开教室,导致每天额外的80分钟户外时间 187 。与没有ROC干预的对照学校相比,该计划在1年后导致近视事件减少了53%。在群集随机广州户外活动纵向试验(GOAL)中,在一天结束时增加了40分钟的户外时间,与对照组学校 12 相比,3年内近视事件减少了23%。ROC和GOAL研究的结果似乎表明,户外暴露和近视发病率降低之间存在剂量反应趋势。另一项以学校为基础的户外推广计划的群集随机试验有效地减少了近视或非近视儿童的近视进展,即使在中等光线强度下,如在走廊或树下 13 。然而,在台湾开展的一项教育家长课外户外活动的好处的运动和一项与家人一起进行的基于激励的户外活动并没有对增加户外时间产生显著影响 12,188 。 值得注意的是,在台湾进行的一项为期15年的研究(天天120计划)鼓励学校允许学生每天花2小时在户外,并证明了5#学龄儿童视力下降(与近视高度相关)患病率增加的长期趋势的逆转。这一发现表明,增加户外时间的学校政策可能是保持视力的直接有效的方法。建议增加每天2-3小时的户外活动时间。这一建议已被新加坡的近视预防战略和中国大陆的近视预防计划 189 采纳。
Management 管理
Optical interventions 光学介入
The use of optical devices for myopia management has many advantages as they are readily available, affordable, well tolerated, enable the viewer to immediately appreciate the benefit of improved vision and can be used by very young children (Fig. 6). Standard single-vision spectacles or contact lenses are the mainstay of managing myopia where the primary goal is to improve distance visual acuity.
使用光学设备进行近视管理具有许多优点,因为它们容易获得、负担得起、耐受性好,使观看者能够立即体会到改善视力的益处,并且可以由非常小的儿童使用(图6)。标准的单视眼镜或隐形眼镜是治疗近视的主要手段,其主要目标是提高远距离视力。
图6:用于视力矫正或近视控制的光学干预策略。

The goal of myopia treatment is to reduce the risk of higher levels of myopia. Early intervention is critical and standard single vision spectacles or contact lenses are the mainstay of management of myopia. Differing kinds of spectacle-based lenses are available, including executive bifocals, progressive addition spectacles and lenses with peripheral defocus management. Contact lens-based approaches include soft contact lenses and orthokeratology lenses and differing designs can correct and slow myopia progression. Other strategies, such as refractive surgery, are available for adults with stable myopia and provide improved convenience and cosmesis by eliminating the use of optical lenses.
近视治疗的目标是降低高度近视的风险。早期干预是至关重要的,标准的单视眼镜或隐形眼镜是近视治疗的主要手段。有不同种类的基于眼镜的镜片可供选择,包括行政双光眼镜、渐进附加眼镜和具有外围散焦管理的镜片。基于隐形眼镜的方法包括软性隐形眼镜和角膜矫正术镜片,不同的设计可以矫正和减缓近视的发展。其他策略,如屈光手术,可用于患有稳定近视的成年人,并通过消除光学镜片的使用来提供改进的便利性和美容。
Single-vision optical lenses correct the myopic refractive error but do not address the underlying problem of elongation of the eye and myopia progression. Thus, the re-assessment of the refractive error at regular intervals (6-monthly to 12-monthly) and lens changes are required to restore normal vision. Although full correction does not slow myopia, in some trials, under-correction (that is, providing less than the required optical power to correct for the refractive error) further worsens myopia progression by up to 30%190,191,192. Moreover, depending on the amount of under-correction employed, visual acuity may be reduced.
单视觉光学镜片矫正近视屈光不正,但不能解决眼睛伸长和近视发展的潜在问题。因此,需要定期(6个月至12个月)重新评估屈光不正并更换晶状体以恢复正常视力。虽然完全矫正不会减缓近视,但在一些试验中,矫正不足(即,提供少于矫正屈光不正所需的光焦度)会在0#时进一步恶化近视进展高达30%。此外,根据所采用的矫正不足的量,视力可能会降低。
As mentioned in the regulation of eye growth, animal studies demonstrate that hyperopic defocus stimulates axial elongation whereas myopic defocus decreases the rate of axial elongation82,118,119. In addition to the optical correction of myopia, lenses (myopia control lenses) are also used to control the progression of myopia based on the hyperopic and myopic defocus mechanism. Myopic defocus stimulation can be imposed at the peripheral retina due to the retinal shape or at the central retina due to a lag in accommodation118,120. Indeed, in RCTs and group-matched clinical trials, several spectacles, soft contact lenses and orthokeratology lenses designed to reduce hyperopic defocus at the retina and/or to induce simultaneous myopic defocus were effective in slowing the progression of myopia193,194,195,196,197,198,199,200,201,202,203,204,205,206,207. Early-generation myopia control lenses, such as bifocal spectacles, aimed to reduce accommodative lag197 whereas new lens types have been designed to reduce peripheral retinal defocus199. These spectacles and contact lenses vary in lens features and patterns of use but essentially have two distinct regions with respect to optical power: one region with a negative optical power that corrects for the refractive error of the eye for distance and a second region with aspects that are relatively more positive than the distance portion to reduce hyperopic defocus and/or impose myopic defocus. Orthokeratology lenses are worn only overnight to reshape or flatten the wearer’s cornea, altering the refractive power of the eye. The fundamental design of these lenses incorporates a central zone that is fitted flatter than the central cornea to achieve the flattening effect. The induced corneal shape results in a retinal image profile with reduced hyperopic defocus at the peripheral retina but the exact mechanisms underlying efficacy remain unclear.
如《眼睛生长的调节》中所述,动物研究表明,远视散焦刺激轴向伸长,而近视散焦降低轴向伸长率 82,118,119 。除了近视的光学矫正之外,还使用基于远视和近视散焦机制的镜片(近视控制镜片)来控制近视的进展。由于视网膜形状,可以在周边视网膜处施加近视散焦刺激,或者由于调节延迟 118,120 ,可以在中央视网膜处施加近视散焦刺激。事实上,在RCT和组匹配临床试验中,设计用于减少视网膜远视散焦和/或诱导同时近视散焦的几种眼镜、软性隐形眼镜和角膜矫正术镜片在减缓近视进展方面是有效的 193,194,195,196,197,198,199,200,201,202,203,204,205,206,207 。早期近视控制镜片,如双焦点眼镜,旨在减少3#时的调节滞后,而新的镜片类型已被设计成减少4#时的周边视网膜散焦。这些眼镜和隐形眼镜在镜片特征和使用模式上有所不同,但基本上具有两个关于光焦度的不同区域:一个区域具有负光焦度,用于校正眼睛对距离的屈光不正,而第二区域具有比距离部分相对更正的方面,以减少远视散焦和/或施加近视散焦。角膜矫正术镜片仅佩戴过夜,以重塑或压平佩戴者的角膜,改变眼睛的屈光力。这些镜片的基本设计结合了比中央角膜更平的中心区域,以实现展平效果。 诱导的角膜形状导致周边视网膜远视散焦减少的视网膜图像轮廓,但功效背后的确切机制仍不清楚。
Evidence suggests that approaches using myopia control contact lenses seemed to be more effective at slowing myopia (25–79% control on the degree of myopia progression) than spectacle-based myopia control lenses (3–34% efficacy in myopia control). This difference may be due to off-axis gazing and eye movements with spectacle lenses. This off-axis of the treatment zone in spectacle lenses may disrupt the signal at the retina208. Furthermore, progressive addition spectacles (also known as multifocal or varifocal lenses) and bifocals, which were initially designed for presbyopia correction with full correction at the top of the lenses and additional power at the bottom of the lenses, require the wearer to be compliant and view through the inferior portion of the lens (where the relative plus power is positioned) for near-based tasks and non-compliance may adversely affect efficacy. However, a new design that comprises multiple segments of relatively positive power positioned in an annulus in the mid-peripheral portion of the spectacle lens resulted in 62% slower axial length change over 2 years than single-vision spectacle lenses207.
有证据表明,使用近视控制隐形眼镜的方法在减缓近视方面似乎比基于眼镜的近视控制镜片(在近视控制方面的功效为3-34%)更有效(对近视发展程度的控制为25-79%)。这种差异可能是由于离轴凝视和眼镜镜片的眼球运动。眼镜镜片中治疗区的这种离轴可能会破坏视网膜 208 处的信号。此外,渐进附加眼镜(也称为多焦点或变焦镜片)和双光眼镜,最初设计用于老花眼矫正,在镜片顶部具有完全矫正,在镜片底部具有额外的光焦度,要求佩戴者顺从并通过镜片的下部(相对正光焦度位于此处)观看近距离任务,不顺从可能对功效产生不利影响。然而,一种新的设计包括位于眼镜镜片中周边部分的环中的多个相对正的光焦度段,导致在2年内比单视眼镜镜片 207 的轴向长度变化慢62%。
Soft contact myopia control lenses are multifocal. Several lens designs on the basis of centre-distance, centre-near and extended depth of focus principles demonstrated an effect on myopia control, but centre-distance designs have been most frequently used as the central portion corrects for the refractive error of the eye and enables good vision193,200,201,203,204,205,206. A 3-year randomized trial proved that higher add-power (+2.50 D) had a statistically significant better efficacy on myopia control than medium add-power (+1.50 D) and single-vision contact lenses209.
软接触近视控制镜片是多焦点的。基于中心距、中心近和扩展焦深原理的几种镜片设计证明了对近视控制的效果,但是中心距设计最常用于中央部分矫正眼睛的屈光不正并实现良好的视力 193,200,201,203,204,205,206 。一项为期3年的随机试验证明,与中等增倍率(+1.50 D)和单视隐形眼镜 209 相比,较高增倍率(+2.50 D)对近视控制具有统计学上显著更好的疗效。
With any myopia control approach, the goal is to reduce the risk of high levels of myopia, especially worse than −5.00 D; thus, early intervention is essential. Children as young as 8 years can be fitted with myopia control contact lenses but younger children may need to wear spectacles193,210,211. The initial lens prescription should be based on cycloplegic refraction but should be re-evaluated every 6 to 12 months. If progression is not sufficiently controlled, guidelines recommend a change to a different treatment or augmentation with combination strategies212.
任何近视控制方法的目标都是降低高度近视的风险,尤其是比5.00 D更严重的近视;因此,早期干预至关重要。8岁的儿童可以佩戴近视控制隐形眼镜,但更小的儿童可能需要佩戴眼镜 193,210,211 。最初的晶状体处方应基于睫状肌麻痹性屈光,但应每6至12个月重新评估一次。如果进展没有得到充分控制,指南建议改变不同的治疗或联合策略的增强 212 。
Although optical strategies have shown success in slowing myopia in young individuals with progressive myopia, the exact mechanism underlying their effectiveness remains uncertain. Very few data beyond 1–2 years exist for many strategies and the longest study duration is 5 years for orthokeratology; thus, the long-term effectiveness of these treatments is unknown. Some evidence suggests that there is no myopic rebound with optical strategies but this has not been systematically addressed213. In addition, the use of overnight wear soft contact lenses and orthokeratology is associated with a small but significant risk of developing sight-threatening complications such as infectious keratitis, for which the annual incidence per 10,000 wearers increases from 1–5 in individuals who wear lenses during the day to at least 20 in individuals who wear lenses overnight214.
尽管光学策略已经显示出在患有进行性近视的年轻个体中减缓近视的成功,但是其有效性背后的确切机制仍然不确定。许多策略很少有超过1-2年的数据,角膜矫正术的最长研究持续时间为5年;因此,这些治疗的长期有效性尚不清楚。一些证据表明,光学策略没有近视反弹,但这还没有得到系统的解决 213 。此外,通宵佩戴软性隐形眼镜和角膜矫正术的使用与发展威胁视力的并发症(如传染性角膜炎)的微小但显著的风险相关,对于传染性角膜炎,每10,000名佩戴者的年发病率从白天佩戴镜片的个体的1-5增加到通宵佩戴镜片的个体的至少20 214 。
Pharmacological interventions
药物干预
Pharmacological interventions for myopia control include the non-specific anti-muscarinic antagonist atropine and the M1 receptor-specific antagonist pirenzepine215,216. Of note, the use of atropine and other pharmacological interventions still necessitates the wearing of glasses in children. Atropine is the most widely studied agent in this indication, including many retrospective cohort studies and RCTs. A meta-analysis of four RCTs demonstrated that the daily use of eye drops with a high dose (0.5–1.0%) of atropine slowed progression by 0.68 D per year compared with the daily use of low dose (0.1% and 0.01%) atropine, which had an effect of 0.53 D per year217. Another meta-analysis of the same four RCTs and seven cohort studies had similar findings, reporting a 0.54 D per year and 0.35 D per year effect in Asian and European children, respectively218. Moreover, another study of seven RCTs and nine cohort studies demonstrated an effect of 0.50 D per year for low-dose (0.01%), 0.57 D per year for moderate-dose (>0.01% to <0.5%) and 0.62 D per year for high-dose atropine (0.5–1.0%), respectively, with a pooled effect size of 2.67 (95% CI 1.46–3.88) in the RCTs and 1.30 (95% CI 0.61–1.98) in the cohort studies219.
控制近视的药物干预包括非特异性抗毒蕈碱拮抗剂阿托品和M1受体特异性拮抗剂哌仑西平 215,216 。值得注意的是,使用阿托品和其他药物干预仍然需要儿童佩戴眼镜。阿托品是该适应症中研究最广泛的药物,包括许多回顾性队列研究和RCT。一项对四项随机对照试验的荟萃分析表明,与每天使用低剂量(0.1%和0.01%)阿托品(每年0.53天)的效果相比,每天使用高剂量(0.5-1.0%)阿托品的滴眼液每年可减缓0.68天的进展。对相同的四项随机对照试验和七项队列研究的另一项荟萃分析有类似的发现,报告亚洲和欧洲儿童每年分别有0.54 D和0.35 D的效应 218 。此外,另一项由七项随机对照试验和九项队列研究组成的研究表明,低剂量阿托品(0.01%)、中剂量阿托品(>0.01%至<0.5%)和高剂量阿托品(0.5-1.0%)的影响分别为每年0.50天、每年0.57天和每年0.62天,随机对照试验和队列研究的合并影响大小分别为2.67(95%CI 1.46-3.88)和1.30(95%CI 0.61-1.98)。
In terms of effect on axial length growth, a slowing of −0.21 mm per year has been observed for 0.1–1% atropine treatment and −0.15 mm per year for 0.01% atropine treatment217. An effect of −0.27 mm per year for higher doses and a pooled effect size of 3.67 (95% CI 1.85–5.50) and 0.68 (95% CI 0.08–1.27) for higher and lower doses, respectively, was reported in another study219. Overall, low-dose atropine (0.01%) seemed to be almost as effective as higher doses after 2 years of treatment and caused less pupil dilation (1.0 mm versus 3.5 mm for 0.5% atropine), less loss of accommodation (4D versus 11D for 0.5% atropine) and was less likely to cause a myopic rebound when stopped220,221,222,223. In 2019, the Low-concentration Atropine for Myopia Progression (LAMP) study demonstrated a dose–response effect of atropine, even at low doses224. In this study, mean SE changed by −0.27 D, −0.46 D, −0.59 D and −0.81 D and mean AL changed by 0.20 mm, 0.29 mm. 0.36 mm and 0.41 mm in children treated with 0.05%, 0.025% and 0.01% atropine and placebo, respectively, for a 1-year period. This trend continued in the second study year with a marked reduction in SE in children who had been in the placebo group and changed to 0.05% atropine224,225. Of note, although there was statistically less SE change in children receiving placebo than in those receiving 0.01% atropine at 1 year (P < 0.006), there was no statistical difference in AL (P = 0.180), perhaps because the low concentration of atropine was not fully controlling the myopia. A myopic rebound may occur, especially when high-dose atropine has been stopped abruptly in children <12 years of age221,226. The risk of rebound was much lower for low-dose atropine (0.01) and was the most effective treatment over 5 years in the Atropine for Treatment of Myopia (ATOM2) study221.
就对轴长生长的影响而言,在0#时,观察到0.1-1%阿托品治疗时每年减速0.21毫米,0.01%阿托品治疗时每年减速0.15毫米。另一项研究 219 报告了较高剂量每年0.27毫米的效应,较高剂量和较低剂量的合并效应大小分别为3.67(95%CI 1.85-5.50)和0.68(95%CI 0.08-1.27)。总体而言,在2年的治疗后,低剂量阿托品(0.01%)似乎与高剂量一样有效,并且引起更少的瞳孔扩张(1.0毫米对0.5%阿托品的3.5毫米),更少的调节损失(4D对0.5%阿托品的11D),并且当在2#停止时不太可能引起近视反弹。2019年,低浓度阿托品治疗近视进展(LAMP)研究证明了阿托品的剂量反应效应,即使在低剂量 224 下也是如此。在这项研究中,平均硒变化了0.27天、0.46天、0.59天和0.81天,平均铝变化了0.20毫米、0.29毫米。分别接受0.05%、0.025%和0.01%阿托品和安慰剂治疗1年的儿童为0.36 mm和0.41 mm。这一趋势在第二个研究年度继续,安慰剂组儿童的SE显著降低,并改为0.05%阿托品 224,225 。值得注意的是,尽管在1年时接受安慰剂的儿童的硒变化在统计学上小于接受0.01%阿托品的儿童(P<0.006),但AL没有统计学差异(P=0.180),这可能是因为低浓度的阿托品没有完全控制近视。可能会出现近视反弹,尤其是当12岁以下儿童突然停用高剂量阿托品时 221,226 。低剂量阿托品的反弹风险低得多(0。01)并且是阿托品治疗近视(ATOM2)研究 221 中超过5年的最有效治疗。
Photophobia and near blur are the most common adverse effects of atropine treatment. Photophobia was reported in 6.5% of individuals who received a low dose (0.01%), in 17.5% of those who received a moderate dose (0.01–0.5%) and in 43.1% of those who received a high dose (1%)219. In addition, a reduction in near vision was noted in 2.3%, 11.9% and 11.6% of individuals who received low-dose, moderate-dose and high-dose atropine, respectively. The other most common ocular adverse effect was an allergic reaction, which occurred in 0–4% participants in a range of studies for various doses219,221,227,228,229. Little effect, at least in the short term (1–2 years), was noted for intraocular pressure change228,230,231, biological lens function223,231 and retinal function232,233.
畏光和近模糊是阿托品治疗最常见的副作用。在接受低剂量(0.01%)的个体中有6.5%报告了畏光,在接受中等剂量(0.01-0.5%)的个体中有17.5%报告了畏光,在接受高剂量(1%)的个体中有43.1%报告了畏光。此外,在接受低剂量、中剂量和高剂量阿托品治疗的个体中,分别有2.3%、11.9%和11.6%的个体的近视下降。另一个最常见的眼部不良反应是过敏反应,在一系列不同剂量 219,221,227,228,229 的研究中,0-4%的参与者出现过敏反应。至少在短期(1-2年)内,眼内压变化 228,230,231 、生物晶状体功能 223,231 和视网膜功能 232,233 几乎没有影响。
The exact mechanism of how antimuscarinic antagonists work234 and their optimal use (dose and regime) are still unknown. Of note, studies suggest an additive effect when low-dose atropine is combined with orthokeratology lenses235,236. In a study in 72 children who were either treated with orthokeratology lenses only or in combination with 0.01% atropine, AL increased by 0.40 mm versus 0.29 mm, respectively, over a 2-year period, with a better effect in children with lower myopia237. However, the effects of combining pharmacological agents with orthokeratology treatment are still unknown. There has been a reluctance to prescribe high-dose atropine owing to its adverse effects and potential long-term risks, but the discovery that low-dose atropine (0.01–0.05%) could also slow myopia progression by 30–70%220,221,222,224,238 with very few adverse effects (alone or in combination with other treatments, for example, other optical myopia control treatment such as multi-focal lenses or contact lens) has resulted in a renewed interest in this therapeutic agent.
抗毒蕈碱拮抗剂在0#起作用的确切机制及其最佳使用(剂量和方案)仍然未知。值得注意的是,研究表明,当低剂量阿托品与角膜矫正术镜片 235,236 联合使用时,会产生叠加效应。在一项对72名仅接受角膜矫正术镜片治疗或与0.01%阿托品联合治疗的儿童的研究中,在2年的时间里,AL分别增加了0.40 mm和0.29 mm,在2#的低近视儿童中效果更好。然而,将药物与角膜矫正术治疗相结合的效果仍然未知。由于高剂量阿托品的副作用和潜在的长期风险,人们不愿意开高剂量阿托品的处方,但发现低剂量阿托品(0.01-0.05%)也可以将近视进展减缓30-70% 220,221,222,224,238 且副作用非常少(单独使用或与其他治疗方法联合使用,例如其他光学近视控制治疗方法,如多焦点镜片或隐形眼镜),导致了对这种治疗剂的新兴趣。
Surgical treatment of myopia
近视的外科治疗
The aim of refractive surgery is to correct the refractive error in adults with stable myopia and reduce their dependence on corrective aids. Surgical options can be broadly classified into keratorefractive procedures or intraocular procedures239. Keratorefractive procedures involve the use of an excimer or femtosecond laser to alter the curvature of the cornea, whereas intraocular procedures involve the use of intraocular lenses to correct the refractive error. Current keratorefractive procedures include laser in situ keratomileusis (LASIK), surface ablation and small incision lenticular extraction (SMILE)240. Intraocular procedures include phakic intraocular lens (PIOL) implantation and cataract surgery.
屈光手术的目的是矫正稳定型近视成人的屈光不正,减少他们对矫正辅助设备的依赖。手术选择可以大致分为角膜屈光手术或眼内手术 239 。角膜屈光手术包括使用准分子或飞秒激光来改变角膜的曲率,而眼内手术包括使用人工晶状体来矫正屈光不正。目前的角膜屈光手术包括激光原位角膜磨镶术(LASIK)、表面消融术和小切口晶状体摘除术(SMILE) 240 。眼内手术包括有晶状体眼人工晶状体(PIOL)植入和白内障手术。
Keratorefractive procedures
角膜屈光手术
LASIK is currently the most popular refractive surgery procedure owing to its excellent efficacy on correcting low, moderate and high myopia with and without astigmatism, quick visual recovery, high predictability on postoperative outcome, and low rate of complications241,242. It involves the creation of a corneal flap with the use of either a microkeratome or femtosecond laser243,244 and the subsequent use of an excimer laser to alter the curvature of the cornea. In general, LASIK is efficacious, predictable and safe242,245 and results in quick visual recovery with minimal postoperative discomfort. However, complications related to corneal flap and the occurrence of postoperative dry eyes are potential problems in LASIK. Preoperative topography assessment to ensure sufficient post-residual stromal thickness and to exclude signs of corneal weakness is important to reduce the risk of corneal ectasia246,247.
LASIK是目前最受欢迎的屈光手术,因为它对矫正伴有或不伴有散光的低度、中度和高度近视具有优异的疗效,视力恢复快,术后结果可预测性高,并发症发生率低。它包括使用微型角膜刀或飞秒激光 243,244 制作角膜瓣,随后使用准分子激光改变角膜曲率。总的来说,LASIK是有效的、可预测的和安全的,并且可以快速恢复视力,术后不适最小。然而,与角膜瓣相关的并发症和术后干眼症的发生是LASIK的潜在问题。术前地形图评估以确保足够的残留后基质厚度并排除角膜薄弱的迹象对于降低角膜扩张的风险非常重要 246,247 。
Surface ablation involves the removal of the corneal epithelium and the subsequent use of an excimer laser to alter the curvature of the cornea. This approach has the advantage of not requiring the creation of a corneal flap and is less likely to induce dry eyes after treatment than LASIK. Several options to remove the epithelium exist, including photorefractive keratectomy using mechanical removal248, epipolis laser in situ keratomileusis using a special microkeratome249,250, laser-assisted subepithelial keratectomy using alcohol251 and transepithelial photorefractive keratectomy using an excimer laser252. The outcomes of surface ablation are similar to those of LASIK, but the removal of the corneal epithelium can result in more patient discomfort after surgery during recovery of the corneal epithelium248,253. In addition, surface ablation has a risk of haze formation, especially in patients with high degrees of myopia; mitomycin can be used as an adjuvant treatment during surgery to reduce this risk254,255. Currently, surface ablation is indicated for patients with relatively thinner corneas and those who do not want the risk of corneal flap complications.
表面消融包括去除角膜上皮,随后使用准分子激光来改变角膜的曲率。这种方法的优点是不需要产生角膜瓣,并且在治疗后比LASIK更不容易引起干眼症。存在几种去除上皮的选择,包括使用机械去除的屈光性角膜切除术 248 、使用特殊微型角膜刀的epipolis激光原位角膜磨镶术 249,250 、使用酒精的激光辅助上皮下角膜切除术 251 和使用准分子激光的跨上皮屈光性角膜切除术 252 。表面消融的结果与LASIK相似,但角膜上皮的去除会导致术后角膜上皮恢复期间患者更不适 248,253 。此外,表面消融有形成雾霾的风险,尤其是在高度近视的患者中;丝裂霉素可以在手术中作为辅助治疗,以降低这种风险 254,255 。目前,表面消融术适用于角膜相对较薄的患者和不希望有角膜瓣并发症风险的患者。
SMILE surgery involves the use of a femtosecond laser to create a corneal lenticule tissue, which is subsequently removed though a 2.5–4 mm corneal incision leading to a change in the corneal curvature. SMILE is a flapless corneal laser procedure with minimal postoperative discomfort256,257 and dry eye syndrome may be less severe than with LASIK258. SMILE seems to be efficacious, safe and with a more predictable outcome259,260 but refractive error correction is limited to myopia that is less severe than −12 D. SMILE may also reduce biomechanical weakness in the cornea compared with LASIK261 but corroborating this hypothesis requires longer-term studies.
微笑手术包括使用飞秒激光来创建角膜微透镜组织,随后通过2.5-4 mm的角膜切口将其移除,从而改变角膜曲率。SMILE是一种无瓣角膜激光手术,术后不适最小 256,257 ,干眼症可能没有LASIK 258 严重。SMILE似乎是有效的、安全的,并且具有更可预测的结果 259,260 ,但是屈光不正矫正仅限于不到12 D的近视。与LASIK 261 相比,SMILE还可以减少角膜的生物力学弱点,但是证实这一假设需要更长期的研究。
Intraocular procedures 眼内手术
PIOL surgery requires the implantation of an intraocular lens in the anterior segment of the eye to correct refractive errors. PIOLs can either be angle-supported anterior chamber lenses, iris-supported anterior chamber lenses or sulcus-supported posterior chamber lenses262. PIOLs have the advantage of correcting very high degrees of myopia and can be used in patients with thin corneas or abnormal corneal topographies263. Currently, most PIOL surgeries involve the use of sulcus-supported posterior chamber PIOLs owing to the much lower risk of corneal endothelial damage and pupil ovalization (a complication that changes the pupil shape from round to oval)264 and can also correct astigmatism at the same time. Although PIOLs are effective in correcting myopia265, this procedure is associated with more severe intraocular risks than keratorefractive procedures such as infective endophthalmitis. As PIOL surgery involves the insertion of an additional lens in the anterior segment, there must be sufficient space from the endothelium to the anterior lens surface266. Posterior chamber PIOLs have been associated with higher long-term risks of cataract formation267,268 and glaucoma than usual for the normal eye268. Thus, patients with PIOLs must be assessed regularly (once per year).
PIOL手术需要在眼睛的前段植入人工晶状体来矫正屈光不正。PIOLs可以是角度支撑的前房镜片、虹膜支撑的前房镜片或沟支撑的后房镜片 262 。PIOLs具有矫正非常高程度近视的优点,可用于角膜薄或角膜地形图异常的患者 263 。目前,大多数PIOL手术涉及使用沟支撑的后房PIOL,因为角膜内皮损伤和瞳孔椭圆化(一种将瞳孔形状从圆形变为椭圆形的并发症) 264 的风险低得多,并且还可以同时矫正散光。虽然PIOLs在矫正近视 265 方面是有效的,但这种手术比角膜屈光手术(如感染性眼内炎)具有更严重的眼内风险。由于PIOL手术涉及在前段插入额外的晶状体,因此从内皮到前晶状体表面必须有足够的空间 266 。与正常眼睛相比,后房PIOLs与白内障形成(5#)和青光眼(6#)的长期风险更高相关。因此,必须定期(每年一次)评估PIOLs患者。
For patients with myopia and cataracts, cataract surgery with intraocular lens implantation can correct refractive errors and should therefore be the surgery of choice in these patients if they want to correct their refractive error. Thorough ocular biometry is essential to ensure accurate intraocular lens calculation. Clear lens extraction with intraocular lens implantation for patients who do not have cataracts is controversial, although this procedure can correct refractive errors in patients with myopia who cannot undergo other refractive surgery procedures; however, the risks of intraocular complications and the loss of accommodation in a patient with healthy eyes (those without cataracts) makes clear-lens extraction very controversial269,270.
对于近视和白内障患者,人工晶状体植入的白内障手术可以矫正屈光不正,因此如果他们想要矫正屈光不正,应该是这些患者的首选手术。全面的眼部生物测量对于确保准确的人工晶状体计算至关重要。对没有白内障的患者进行透明晶状体摘除和人工晶状体植入是有争议的,尽管这种手术可以矫正不能接受其他屈光手术的近视患者的屈光不正;然而,眼睛健康的患者(没有白内障的患者)的眼内并发症和调节能力丧失的风险使得透明晶状体摘除非常有争议 269,270 。
Quality of life 生活质量
Understanding the effects of myopia on quality of life and the effectiveness of treatments from the patient’s perspective has become a critical focus of research and clinical practice, especially with the shift from a volume-focused to a value-focused health-care system271. This approach is particularly important given the high prevalence of myopia272, the debilitating visual effects, particularly if myopia is uncorrected or under-corrected273, the increased risk profile for sight-threatening complications such as in pathologic myopia51,274,275,276, and the range of potential corrective therapies available242,277. For instance, the large epidemiological Singapore Malay Eye Study showed that uncorrected myopia resulted in permanent blurring of vision and therefore in difficulties with visual tasks such as reading street signs and watching television278. In addition, a substantial proportion of individuals with uncorrected or under-corrected myopia have described frequent bouts of anger, frustration and/or depressive symptoms related to their inability to carry out simple visual tasks279 as well as poor sleep quality280. Moreover, the quality of life effect of under-corrected high myopia is comparable with that of keratoconus, a vision-threatening corneal dystrophy281. However, compared with other ocular diseases, uncomplicated myopia can be easily and fully corrected with a range of optical and surgical interventions282,283,284. Despite the excellent visual acuity outcomes offered by these interventions, they often have considerable quality of life drawbacks, including dry eyes (in contact lens wearers and after LASIK)285,286, inconvenience resulting from participants’ refractive corrections (for example, glasses sliding down noses) and financial concerns (for example, long-term cost of purchasing contact lenses)287. In addition, population-based data from Singapore indicated that pathologic myopia was associated with a significant reduction in vision-specific functioning59; patients who developed pathologic myopia over a 6-year period experienced substantial decrements in reading, mobility and emotional well-being domains of vision-related quality of life that were independent of visual impairment compared with patients who did not develop pathologic myopia59.
从患者的角度了解近视对生活质量和治疗效果的影响已经成为研究和临床实践的关键焦点,特别是随着医疗保健系统从注重数量向注重价值的转变。考虑到近视 272 的高患病率、使人虚弱的视觉效应,特别是如果近视未矫正或矫正不足 273 、威胁视力的并发症(如病理性近视 51,274,275,276 )的风险增加以及可用的潜在矫正疗法的范围 242,277 ,这种方法尤其重要。例如,大型流行病学新加坡马来人眼科研究表明,未矫正的近视导致永久性视力模糊,因此在视觉任务方面存在困难,如阅读街道标志和看电视 278 。此外,相当比例的未矫正或矫正不足的近视患者描述了与他们无法执行简单视觉任务 279 以及睡眠质量差 280 相关的频繁发作的愤怒、沮丧和/或抑郁症状。此外,矫正不足的高度近视的生活质量影响与圆锥角膜相当,圆锥角膜是一种威胁视力的角膜营养不良 281 。然而,与其他眼部疾病相比,无并发症的近视可以通过一系列的光学和手术干预来轻松和完全地矫正 282,283,284 。 尽管这些干预措施提供了出色的视力结果,但它们往往有相当大的生活质量缺陷,包括干眼症(隐形眼镜佩戴者和LASIK手术后) 285,286 ,参与者屈光矫正造成的不便(例如,眼镜滑下鼻子)和财务问题(例如,购买隐形眼镜的长期成本) 287 。此外,来自新加坡的基于人群的数据表明,病理性近视与视觉特异性功能的显著降低有关 59 ;与未发生病理性近视的患者相比,在6年内发生病理性近视的患者在阅读、活动能力和视觉相关生活质量的情绪健康领域经历了显著下降,这些领域与视力障碍无关 59 。
Patient difficulties can be quantified using patient-reported outcome measures (PROMs). Data from PROMs, in the form of questionnaires, are valuable as they can be used to improve clinical care and patient–provider relationships as well as to inform comparative effectiveness research and value-based care models288. The importance of evaluating PROMs has been recognized by many regulatory authorities around the world and their assessment is required in clinical trials that evaluate new treatments. Thus, high-quality, comprehensive PROMs are needed to accurately assess the substantial and wide-ranging effects of myopia and its associated corrective therapies on quality of life. However, most popular myopia-specific PROMs, including the Quality of Life Impact of Refractive Correction (QIRC)289 and the National Eye Institute Refractive Quality of Life (NEI-RQL)290 questionnaires, have several major shortcomings. First, the number of questions (items) is fixed and responders have to complete all items to achieve an overall summary score. To reduce participant burden, these tools either target only specific subsets of individuals with myopia (for example, those wearing glasses)289 and/or focus on certain aspects of quality of life (for example, activity limitation and symptoms)291. Second, modern psychometric techniques (for example, Rasch analysis) have highlighted several limitations of these questionnaires, including poor validity, reliability and targeting292, which make the comparison of results between studies difficult and limit the comprehensive and nuanced quality of life assessment of patients across the severity spectrum of myopia and its different corrective options.
可以使用患者报告的结果测量(PROMs)来量化患者的困难。问卷形式的PROMs数据非常有价值,因为它们可用于改善临床护理和患者——提供者关系,以及为比较有效性研究和基于价值的护理模式提供信息 288 。评估PROMs的重要性已经被世界各地的许多监管机构所认识,并且在评估新治疗的临床试验中需要对其进行评估。因此,需要高质量、全面的PROMs来准确评估近视及其相关矫正治疗对生活质量的实质性和广泛影响。然而,大多数流行的近视特异性PROMs,包括屈光矫正的生活质量影响(QIRC) 289 和国家眼科研究所屈光生活质量(NEI-RQL) 290 问卷,都有几个主要缺点。首先,问题(项目)的数量是固定的,回答者必须完成所有项目才能获得总的总结分数。为了减轻参与者的负担,这些工具要么只针对近视个体的特定子集(例如,戴眼镜的人) 289 和/或关注生活质量的某些方面(例如,活动限制和症状) 291 。其次,现代心理测量技术(例如Rasch分析)强调了这些问卷的几个局限性,包括效度、信度和目标 292 差,这使得研究之间的结果比较困难,并限制了对近视严重程度谱及其不同矫正选项的患者进行全面和细致入微的生活质量评估。
These limitations can potentially be overcome by sophisticated psychometric methods of instrument (questionnaire) development and validation, namely item banking (IB) and computerized adaptive testing (CAT). An IB is a large pool of items ranked or ‘calibrated’ for difficulty on the same linear scale on the basis of a participant’s response and the use of modern psychometric techniques such as the Rasch analysis293. IBs are operationalized using CAT, a computer-based ‘smart’ technology that selects the items to be administered based on participants’ responses to previous items294. By presenting items from a calibrated IB targeted to a respondent’s ability level, CAT reduces measurement error and test length without sacrificing precision and reliability294. However, IBs and CAT have not been developed to comprehensively assess the impact of myopia, across its severity spectrum and corrective interventions, on quality of life. The mounting public health burden resulting from myopia272, together with related treatments such as LASIK242, require a global effort to incorporate assessment in value-based health-care systems295 as well as a valid CAT to assess myopia and the effectiveness of related corrections in both Asian and Western societies.
这些限制可以通过工具(问卷)开发和验证的复杂心理测量方法来克服,即题库(IB)和计算机化适应性测试(CAT)。IB是根据参与者的反应和现代心理测量技术(如Rasch analysis 293 )的使用,在相同的线性量表上对难度进行排名或“校准”的大型项目池。IBs使用CAT进行操作,CAT是一种基于计算机的“智能”技术,它根据参与者对先前项目 294 的反应来选择要管理的项目。通过根据受访者的能力水平展示校准IB中的项目,CAT减少了测量误差和测试长度,而不牺牲精度和可靠性 294 。然而,IBs和CAT还没有被开发来全面评估近视的严重程度和矫正干预对生活质量的影响。近视 272 以及LASIK 242 等相关治疗导致的日益增加的公共卫生负担,需要全球努力将评估纳入基于价值的医疗保健系统 295 以及有效的CAT,以评估亚洲和西方社会的近视和相关矫正的有效性。
Outlook 展望
Preventing the onset of myopia and slowing its progression are recognized as priority areas for myopia-related public health interventions. Treatments of myopia have partial efficacy but they often require long-term use and may have adverse effects. A risk-triaging system that helps identify those patients at greatest risk of developing high myopia by adulthood could be helpful to improve the targeting of treatments. Additionally, a reduction of one dioptre of myopia would benefit patients by reducing the risk of developing myopic maculopathy6. Thus, myopia control should focus on reducing the risk of developing high myopia in adulthood when the proportion of myopic maculopathy would be exponentially higher.
预防近视的发作和减缓其发展被认为是近视相关公共卫生干预的优先领域。近视的治疗有部分疗效,但它们通常需要长期使用,并可能产生副作用。一个有助于识别成年后患高度近视风险最大的患者的风险分类系统可能有助于提高治疗的针对性。此外,近视减少一屈光度将通过降低发展为近视黄斑病变 6 的风险而使患者受益。因此,近视控制应集中于降低成年期发展为高度近视的风险,此时近视性黄斑病变的比例将呈指数级上升。
The prevention or delay of myopia onset should be the first steps for myopia control. Each year of delay in the age at onset would substantially reduce the chance of developing high myopia in adulthood296. However, effective prevention strategies, in terms of encouraging more time spent outdoors and reducing near-work or educational intensity, require the commitment and involvement of both government and education sectors.
预防或延缓近视发病应是控制近视的首要步骤。发病年龄每延迟一年,成年后患高度近视的几率就会大大降低。然而,有效的预防战略,即鼓励更多的时间花在户外,减少近距离工作或教育强度,需要政府和教育部门的承诺和参与。
On the other hand, for ophthalmic practitioners, properly defining progressive myopia should ideally be the first step in myopia control interventions. Data from population studies and clinical trials suggest that an annual progression of −0.75 D or more can be used as a population norm to define progressive myopia297,298,299. However, in general, the progression of myopia slows with increasing age; therefore, definitions of progressive myopia need to be age specific. Furthermore, myopia progression and axial elongation can occur in spurts, meaning that attempts to identify individual children with a high progression rate need to be based on careful modelling of refractive trajectories in the local population300,301.
另一方面,对于眼科医生来说,正确定义进行性近视应该是近视控制干预的第一步。来自人群研究和临床试验的数据表明,0.75 D或更高的年进展可用作人群标准来定义进行性近视 297,298,299 。然而,一般来说,近视的进展随着年龄的增长而减缓;因此,进行性近视的定义需要有年龄特异性。此外,近视进展和眼轴伸长可以突发发生,这意味着识别具有高进展率的个体儿童的尝试需要基于当地人群中屈光轨迹的仔细建模 300,301 。
The search for additional common and rare genetic variants associated with myopia and its underlying ocular biometric traits will continue through increasingly larger GWAS meta-analyses as well as through important contributions from whole-exome and whole-genome sequencing. In addition, studies evaluating changes in copy number, epigenetics, and gene–gene and G×E interaction analyses will provide a more comprehensive picture of the genetic mechanisms involved in myopia. Population centile curves and prediction models containing multiple risk factors, such as parental myopia, age at myopia onset and environmental factors, have already yielded acceptable predictive outcomes301,302,303,304. Age-specific refraction data and the information on age at myopia onset are currently the best predictors of who will develop high myopia by adulthood305. Genetic susceptibility, assessed through the genotyping of genetic variants identified in GWAS studies, also has the potential to contribute to risk prediction94,96. However, current genetic prediction models have yet to outperform prediction models based on simpler criteria96,300.
通过越来越大的GWAS荟萃分析以及全外显子组和全基因组测序的重要贡献,将继续寻找与近视及其潜在眼部生物特征相关的其他常见和罕见的遗传变异。此外,评估拷贝数、表观遗传学、基因——基因和G × E相互作用分析变化的研究将提供近视相关遗传机制的更全面的图片。包含多种风险因素(如父母近视、近视发病年龄和环境因素)的人口百分位数曲线和预测模型已经产生了可接受的预测结果 301,302,303,304 。年龄特异性屈光数据和近视发病年龄信息目前是谁将在成年后发展为高度近视的最佳预测因素 305 。通过GWAS研究中确定的遗传变异的基因分型评估的遗传易感性也有可能有助于风险预测 94,96 。然而,目前的遗传预测模型尚未优于基于更简单标准的预测模型 96,300 。
The finding that genetic susceptibility to myopia-predisposing lifestyle factors is shared across Asians and Europeans90 offers the prospect that myopia control inventions demonstrated to be effective in one ethnic group will also work in other ethnic groups as long as the lifestyle risk factor is present in both populations.
亚洲人和欧洲人对近视易感生活方式因素的遗传易感性 90 的发现提供了一种前景,即只要生活方式风险因素在两个人群中都存在,在一个种族群体中证明有效的近视控制发明也将在其他种族群体中有效。
New technology has been developed to promote behaviour changes relevant to myopia control. Wearable devices in combination with internet or social network apps designed to encourage outdoor activities are now available. For instance, FitSight comprises a smartwatch with a light sensor and an accompanying smartphone app that logs time spent outdoors and sends feedback to parents and children306. Other similar devices have also been launched, such as Clouclip307, a cloud-based sensor device that attaches to the sides of spectacles, measures reading distance, ambient illuminance, and distinguishes between indoor and outdoor environments. The device provides real-time feedback to children and generates daily reports to parents that help them to quantify environmental risk factors and monitor myopia-related behaviour. However, such a device is useful only for those who have already developed myopia and are wearing spectacles, which may limit its use in the prevention of myopia onset. Studies of G×E interactions should benefit from the precise, quantitative measurements of time outdoors and time engaged in near-work obtained from these new wearable sensors compared with past coarse-grained estimates from questionnaires.
已经开发了新技术来促进与近视控制相关的行为改变。结合互联网或社交网络应用程序的可穿戴设备旨在鼓励户外活动,现已上市。例如,FitSight包括一个带光传感器的智能手表和一个附带的智能手机应用程序,该应用程序记录户外时间,并向父母和孩子发送反馈 306 。其他类似的设备也已经推出,如Clouclip 307 ,这是一种基于云的传感器设备,可以附着在眼镜的两侧,测量阅读距离,环境照度,并区分室内和室外环境。该设备向儿童提供实时反馈,并向父母生成每日报告,帮助他们量化环境风险因素并监控近视相关行为。然而,这种装置仅对那些已经发展成近视并且戴着眼镜的人有用,这可能限制其在预防近视发作中的使用。与过去来自问卷调查的粗粒度估计相比,G × E相互作用的研究应该受益于从这些新的可穿戴传感器获得的户外时间和从事近距离工作的时间的精确、定量测量。
Another behaviour change strategy focuses on minimizing screen time on computers, tablets and smartphones, although current evidence suggests that the role of screen time in myopia development is very limited308. Nevertheless, a restriction on screen time may be of benefit by encouraging children to spend more time outdoors. Optical and pharmacological interventions, such as orthokeratology and low dose atropine, designed to slow myopia progression in children are now being widely adopted.
另一种行为改变策略侧重于最大限度地减少电脑、平板电脑和智能手机上的屏幕时间,尽管目前的证据表明,屏幕时间在近视发展中的作用非常有限 308 。然而,限制屏幕时间可能有利于鼓励孩子们花更多的时间在户外。旨在减缓儿童近视发展的光学和药物干预,如角膜矫正术和低剂量阿托品,现在正被广泛采用。
In conclusion, our ability to synthesize large amounts of information from genetic and other omic levels of data together with input of environment, demographic and lifestyle exposures collected from personal sensors, such as wearable devices, will enable a more nuanced approach to myopia management in the future. Applying artificial intelligence algorithms to these data sources offers a promising avenue for improved public health strategies focusing on the early detection or prevention of myopia and for more effective therapeutic interventions to slow or prevent myopia progression to its damaging extremes.
总之,我们从遗传和其他组学水平的数据中综合大量信息的能力,以及从个人传感器(如可穿戴设备)收集的环境、人口统计和生活方式暴露的输入,将在未来实现更细致入微的近视管理方法。将人工智能算法应用于这些数据源,为改善专注于近视早期检测或预防的公共卫生策略以及更有效的治疗干预提供了一种有希望的途径,以减缓或防止近视发展到其破坏性的极端。
References 参考文献
Modjtahedi, B. S., Ferris, F. L., Hunter, D. G. & Fong, D. S. Public health burden and potential interventions for myopia. Ophthalmology 125, 628–630 (2018).
近视的公共卫生负担和潜在干预措施。眼科学125,628–630(2018)。Morgan, I. G. et al. The epidemics of myopia: aetiology and prevention. Prog. Retin. Eye Res. 62, 134–149 (2018). This study summarized the increasing trend of myopia prevalence and further discussed the implication and possible aetiology of the ‘epidemics’ of myopia.
摩根等人。近视的流行:病因和预防。进步。雷丁。第62、134-149号决议(2018年)。本研究总结了近视患病率的上升趋势,并进一步讨论了近视“流行”的含义和可能的病因。Resnikoff, S. et al. Myopia - a 21st century public health issue. Invest. Ophthalmol. Vis. Sci. 60, Mi–Mii (2019).
近视——21世纪的公共健康问题。投资。眼底镜。维斯。Sci.60、米米(2019)。Young, T. L., Metlapally, R. & Shay, A. E. Complex trait genetics of refractive error. Arch. Ophthalmol. 125, 38–48 (2007).
屈光不正的复杂性状遗传学。拱门。眼底镜。125,38-48(2007).Hashemi, H. et al. The prevalence and risk factors for keratoconus: a systematic review and meta-analysis. Cornea 39, 263–270 (2020).
哈希米,H.等人。圆锥角膜的患病率和危险因素:一项系统综述和荟萃分析。角膜39,263–270(2020)。Bullimore, M. A. & Brennan, N. A. Myopia control: why each diopter matters. Optom. Vis. Sci. 96, 463–465 (2019).
近视控制:为什么每个屈光度都很重要。光学。维斯。Sci.96,463–465(2019).Holden, B. A. et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology 123, 1036–1042 (2016). This study showed the temporal trend of myopia and high myopia prevalence supporting the notion that there will be a very high prevalence of myopia in 2050.
霍尔登,文学学士等人。2000年至2050年全球近视和高度近视的患病率及时间趋势。眼科123,1036–1042(2016)。这项研究显示了近视和高近视患病率的时间趋势,支持了2050年近视患病率将非常高的观点。Mutti, D. O., Mitchell, G. L., Moeschberger, M. L., Jones, L. A. & Zadnik, K. Parental myopia, near work, school achievement, and children’s refractive error. Invest. Ophthalmol. Vis. Sci. 43, 3633–3640 (2002).
父母近视、近距离工作、学校成绩和儿童屈光不正。投资。眼底镜。维斯。Sci.43,3633–3640(2002).Huang, H.-M., Chang, D. S.-T. & Wu, P.-C. The association between near work activities and myopia in children-a systematic review and meta-analysis. PLoS ONE 10, e0140419 (2015).
Jin, J.-X. et al. Effect of outdoor activity on myopia onset and progression in school-aged children in northeast China: the Sujiatun eye care study. BMC Ophthalmol. 15, 73 (2015).
Saxena, R. et al. Prevalence of myopia and its risk factors in urban school children in Delhi: the North India myopia study (NIM study). PLoS ONE 10, e0117349 (2015).
He, M. et al. Effect of time spent outdoors at school on the development of myopia among children in China: a randomized clinical trial. JAMA 314, 1142–1148 (2015). This study is a large RCT and confirmed that outdoor activity significantly prevented myopia onset.
Wu, P. C. et al. Myopia prevention and outdoor light intensity in a school-based cluster randomized trial. Ophthalmology 125, 1239–1250 (2018). This study was the first RCT that confirmed outdoor activity significantly prevented myopia onset and myopia progression even in moderate light intensity.
Saw, S.-M., Carkeet, A. D., Chia, K.-S., Stone, R. A. & Tan, D. T. H. Component dependent risk factors for ocular parameters in Singapore Chinese children. Ophthalmology 109, 2065–2071 (2002).
He, M. et al. Refractive error and visual impairment in urban children in southern China. Invest. Ophthalmol. Vis. Sci. 45, 793–799 (2004).
Yam, J. C. et al. High prevalence of myopia in children and their parents in Hong Kong Chinese population: the Hong Kong children eye study. Acta Ophthalmol. https://doi.org/10.1111/aos.14350 (2020).
Hsu, C.-C. et al. Prevalence and risk factors for myopia in second-grade primary school children in Taipei: a population-based study. J. Chin. Med. Assoc. 79, 625–632 (2016).
Lin, L. L. K., Shih, Y. F., Hsiao, C. K. & Chen, C. J. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann. Acad. Med. Singap. 33, 27–33 (2004).
Yotsukura, E. et al. Current prevalence of myopia and association of myopia with environmental factors among schoolchildren in Japan. JAMA Ophthalmol. 137, 1233–1239 (2019).
Lim, D. H., Han, J., Chung, T., Kang, S. & Yim, H. W. Correction: the high prevalence of myopia in Korean children with influence of parental refractive errors: the 2008–2012 Korean national health and nutrition examination survey. PLoS ONE 13, e0209876 (2018).
Anera, R. G., Soler, M., de la Cruz Cardona, J., Salas, C. & Ortiz, C. Prevalence of refractive errors in school-age children in Morocco. Clin. Exp. Ophthalmol. 37, 191–196 (2009).
Casson, R. J. et al. Exceptionally low prevalence of refractive error and visual impairment in schoolchildren from Lao People’s Democratic Republic. Ophthalmology 119, 2021–2027 (2012).
Dandona, R. et al. Population-based assessment of refractive error in India: the Andhra Pradesh eye disease study. Clin. Exp. Ophthalmol. 30, 84–93 (2002).
Xiang, F. et al. Increases in the prevalence of reduced visual acuity and myopia in chinese children in Guangzhou over the past 20 years. Eye 27, 1353–1358 (2013).
Ding, B.-Y., Shih, Y.-F., Lin, L. L. K., Hsiao, C. K. & Wang, I. J. Myopia among schoolchildren in East Asia and Singapore. Surv. Ophthalmol. 62, 677–697 (2017).
Fan, D. S. et al. Prevalence, incidence, and progression of myopia of school children in Hong Kong. Invest. Ophthalmol. Vis. Sci. 45, 1071–1075 (2004).
Zadnik, K. Myopia development in childhood. Optom. Vis. Sci. 74, 603–608 (1997).
Ip, J. M. et al. Ethnic differences in refraction and ocular biometry in a population-based sample of 11–15-year-old Australian children. Eye 22, 649–656 (2008).
Alrahili, N. H. R. et al. Prevalence of uncorrected refractive errors among children aged 3-10 years in western Saudi Arabia. Saudi Med. J. 38, 804–810 (2017).
Carter, M. J. et al. Visual acuity and refraction by age for children of three different ethnic groups in Paraguay. Arq. Bras. Oftalmol. 76, 94–97 (2013).
Gao, Z. et al. Refractive error in school children in an urban and rural setting in Cambodia. Ophthalmic Epidemiol. 19, 16–22 (2012).
Murthy, G. V. S. et al. Refractive error in children in an urban population in New Delhi. Investig. Ophthalmol. Vis. Sci. 43, 623–631 (2002).
Sapkota, Y. D., Adhikari, B. N., Pokharel, G. P., Poudyal, B. K. & Ellwein, L. B. The prevalence of visual impairment in school children of upper-middle socioeconomic status in Kathmandu. Ophthalmic Epidemiol. 15, 17–23 (2008).
Jung, S. K., Lee, J. H., Kakizaki, H. & Jee, D. Prevalence of myopia and its association with body stature and educational level in 19-year-old male conscripts in Seoul, South Korea. Invest. Ophthalmol. Vis. Sci. 53, 5579–5583 (2012).
Lee, Y. Y., Lo, C. T., Sheu, S. J. & Lin, J. L. What factors are associated with myopia in young adults? A survey study in Taiwan military conscripts. Invest. Ophthalmol. Vis. Sci. 54, 1026–1033 (2013).
Cheng, C. Y., Hsu, W. M., Liu, J. H., Tsai, S. Y. & Chou, P. Refractive errors in an elderly chinese population in Taiwan: the Shihpai eye study. Invest. Ophthalmol. Vis. Sci. 44, 4630–4638 (2003).
Xu, L. et al. Refractive error in urban and rural adult Chinese in Beijing. Ophthalmology 112, 1676–1683 (2005).
Vitale, S., Ellwein, L., Cotch, M. F., Ferris, F. L. 3rd & Sperduto, R. Prevalence of refractive error in the United States, 1999–2004. Arch. Ophthalmol. 126, 1111–1119 (2008).
Midelfart, A., Kinge, B., Midelfart, S. & Lydersen, S. Prevalence of refractive errors in young and middle-aged adults in Norway. Acta Ophthalmol. Scand. 80, 501–505 (2002).
Bar Dayan, Y. et al. The changing prevalence of myopia in young adults: a 13-year series of population-based prevalence surveys. Invest. Ophthalmol. Vis. Sci. 46, 2760–2765 (2005).
Williams, K. M. et al. Increasing prevalence of myopia in Europe and the impact of education. Ophthalmology 122, 1489–1497 (2015).
Chen, M. et al. The increasing prevalence of myopia and high myopia among high school students in Fenghua city, eastern China: a 15-year population-based survey. BMC Ophthalmol. 18, 159 (2018).
Sun, J. et al. High prevalence of myopia and high myopia in 5060 chinese university students in Shanghai. Investig. Ophthalmol. Vis. Sci. 53, 7504–7509 (2012).
Wu, J. F. et al. Refractive error, visual acuity and causes of vision loss in children in Shandong, China. The Shandong children eye study. PLoS ONE 8, e82763 (2013).
Williams, K. M. et al. Prevalence of refractive error in Europe: the European eye epidemiology (E(3)) consortium. Eur. J. Epidemiol. 30, 305–315 (2015).
Jacobsen, N., Jensen, H. & Goldschmidt, E. Prevalence of myopia in Danish conscripts. Acta Ophthalmol. Scand. 85, 165–170 (2007).
French, A. N., Morgan, I. G., Burlutsky, G., Mitchell, P. & Rose, K. A. Prevalence and 5- to 6-year incidence and progression of myopia and hyperopia in Australian schoolchildren. Ophthalmology 120, 1482–1491 (2013).
Willis, J. R. et al. The prevalence of myopic choroidal neovascularization in the United States: analysis of the IRIS(®) data registry and NHANES. Ophthalmology 123, 1771–1782 (2016).
Asakuma, T. et al. Prevalence and risk factors for myopic retinopathy in a Japanese population: the Hisayama study. Ophthalmology 119, 1760–1765 (2012).
Chen, S. J. et al. Prevalence and associated risk factors of myopic maculopathy in elderly Chinese: the Shihpai eye study. Invest. Ophthalmol. Vis. Sci. 53, 4868–4873 (2012).
Vongphanit, J., Mitchell, P. & Wang, J. J. Prevalence and progression of myopic retinopathy in an older population. Ophthalmology 109, 704–711 (2002).
Myrowitz, E. H. Juvenile myopia progression, risk factors and interventions. Saudi J. Ophthalmol. 26, 293–297 (2012).
Fan, D. S., Lai, C., Lau, H. H., Cheung, E. Y. & Lam, D. S. Change in vision disorders among Hong Kong preschoolers in 10 years. Clin. Exp. Ophthalmol. 39, 398–403 (2011).
Lai, Y.-H., Hsu, H.-T., Wang, H.-Z., Chang, S.-J. & Wu, W.-C. The visual status of children ages 3 to 6 years in the vision screening program in Taiwan. J. AAPOS 13, 58–62 (2009).
Choudhury, F. et al. Prevalence and characteristics of myopic degeneration in an adult Chinese American population: the Chinese American eye study. Am. J. Ophthalmol. 187, 34–42 (2018).
Iwase, A. et al. Prevalence and causes of low vision and blindness in a Japanese adult population: the Tajimi study. Ophthalmology 113, 1354–1362 (2006).
Naidoo, K. S. et al. Potential lost productivity resulting from the global burden of myopia: systematic review, meta-analysis, and modeling. Ophthalmology 126, 338–346 (2019).
Seet, B. et al. Myopia in Singapore: taking a public health approach. Br. J. Ophthalmol. 85, 521–526 (2001).
Wong, Y.-L. et al. Prevalence, risk factors, and impact of myopic macular degeneration on visual impairment and functioning among adults in Singapore. Investig. Ophthalmol. Vis. Sci. 59, 4603–4613 (2018).
Liu, H. H. et al. Prevalence and progression of myopic retinopathy in Chinese adults: the Beijing eye study. Ophthalmology 117, 1763–1768 (2010).
Gao, L. Q. et al. Prevalence and characteristics of myopic retinopathy in a rural Chinese adult population: the Handan eye study. Arch. Ophthalmol. 129, 1199–1204 (2011).
Ohno-Matsui, K. et al. International photographic classification and grading system for myopic maculopathy. Am. J. Ophthalmol. 159, 877–883.e7 (2015).
Bez, D. et al. Association between type of educational system and prevalence and severity of myopia among male adolescents in Israel. JAMA Ophthalmol. 137, 1–7 (2019).
Morgan, R. W., Speakman, J. S. & Grimshaw, S. E. Inuit myopia: an environmentally induced “epidemic”? Can. Med. Assoc. J. 112, 575–577 (1975).
He, M., Zheng, Y. & Xiang, F. Prevalence of myopia in urban and rural children in mainland China. Optom. Vis. Sci. 86, 40–44 (2009).
Wong, T. Y., Foster, P. J., Johnson, G. J. & Seah, S. K. Education, socioeconomic status, and ocular dimensions in Chinese adults: the Tanjong Pagar Survey. Br. J. Ophthalmol. 86, 963–968 (2002).
de Jong, P. T. V. M. Myopia: its historical contexts. Br. J. Ophthalmol. 102, 1021–1027 (2018).
Mountjoy, E. et al. Education and myopia: assessing the direction of causality by mendelian randomisation. BMJ 361, k2022 (2018).
Rose, K. A. et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology 115, 1279–1285 (2008).
Guggenheim, J. A. et al. Time outdoors and physical activity as predictors of incident myopia in childhood: a prospective cohort study. Invest. Ophthalmol. Vis. Sci. 53, 2856–2865 (2012).
Guo, Y. et al. Outdoor activity and myopia among primary students in rural and urban regions of Beijing. Ophthalmology 120, 277–283 (2013).
Jones-Jordan, L. A. et al. Time outdoors, visual activity, and myopia progression in juvenile-onset myopes. Invest. Ophthalmol. Vis. Sci. 53, 7169–7175 (2012).
Wu, P. C. et al. Increased time outdoors is followed by reversal of the long-term trend to reduced visual acuity in Taiwan primary school students. Ophthalmology 127, 1462–1469 (2020). This was the first large, long-term real-world population study that showed that outdoor policy reduced the prevalence of reduced visual acuity.
Fulk, G. W., Cyert, L. A. & Parker, D. A. Seasonal variation in myopia progression and ocular elongation. Optom. Vis. Sci. 79, 46–51 (2002).
Ashby, R. S. & Schaeffel, F. The effect of bright light on lens compensation in chicks. Invest. Ophthalmol. Vis. Sci. 51, 5247–5253 (2010).
Feldkaemper, M. & Schaeffel, F. An updated view on the role of dopamine in myopia. Exp. Eye Res. 114, 106–119 (2013).
Guggenheim, J. A. et al. Does vitamin D mediate the protective effects of time outdoors on myopia? Findings from a prospective birth cohort. Invest. Ophthalmol. Vis. Sci. 55, 8550–8558 (2014).
Jacobsen, N., Jensen, H. & Goldschmidt, E. Does the level of physical activity in university students influence development and progression of myopia? – a 2-year prospective cohort study. Invest. Ophthalmol. Vis. Sci. 49, 1322–1327 (2008).
Torii, H. et al. Violet light exposure can be a preventive strategy against myopia progression. EBioMedicine 15, 210–219 (2017).
Moderiano, D. et al. Influence of the time of day on axial length and choroidal thickness changes to hyperopic and myopic defocus in human eyes. Exp. Eye Res. 182, 125–136 (2019).
Wang, Y. et al. Exposure to sunlight reduces the risk of myopia in rhesus monkeys. PLoS ONE 10, e0127863 (2015).
Smith, E. L. III, Kee, C.-S., Ramamirtham, R., Qiao-Grider, Y. & Hung, L.-F. Peripheral vision can influence eye growth and refractive development in infant monkeys. Investig. Ophthalmol. Vis. Sci. 46, 3965–3972 (2005). The first in a series of studies that demonstrated that, contrary to popular belief, visual signals from the fovea (that is, central retina) were not essential for the regulation of ocular growth and that signals from the peripheral retina, probably as a consequence of areal summation, can dominate refractive development.
Sorsby, A. & Fraser, G. R. Statistical note on the components of ocular refraction in twins. J. Med. Genet. 1, 47–49 (1964). The first approach to quantify the coefficient of correlation of different ocular measures in identical and non-identical twins and that suggested that a number of genes with additive effect were inherited in myopia.
Chen, C. Y. et al. Heritability and shared environment estimates for myopia and associated ocular biometric traits: the genes in myopia (GEM) family study. Hum. Genet. 121, 511–520 (2007).
Hammond, C. J., Snieder, H., Gilbert, C. E. & Spector, T. D. Genes and environment in refractive error: the twin eye study. Invest. Ophthalmol. Vis. Sci. 42, 1232–1236 (2001).
Lyhne, N., Sjolie, A. K., Kyvik, K. O. & Green, A. The importance of genes and environment for ocular refraction and its determiners: a population based study among 20–45 year old twins. Br. J. Ophthalmol. 85, 1470–1476 (2001).
Dirani, M. et al. Heritability of refractive error and ocular biometrics: the genes in myopia (GEM) twin study. Invest. Ophthalmol. Vis. Sci. 47, 4756–4761 (2006).
Baird, P. N., Schache, M. & Dirani, M. The genes in myopia (GEM) study in understanding the aetiology of refractive errors. Prog. Retin. Eye Res. 29, 520–542 (2010).
Tedja, M. S. et al. IMI - myopia genetics report. Invest. Ophthalmol. Vis. Sci. 60, M89–M105 (2019).
Verhoeven, V. J. et al. Genome-wide meta-analyses of multiancestry cohorts identify multiple new susceptibility loci for refractive error and myopia. Nat. Genet. 45, 314–318 (2013). The first large international GWAS conducted by the CREAM, based on over 37,000 individuals from 32 European and Asian studies, identified 16 new genetic loci, of which some were shared across ethnicities.
Kiefer, A. K. et al. Genome-wide analysis points to roles for extracellular matrix remodeling, the visual cycle, and neuronal development in myopia. PLoS Genet. 9, e1003299 (2013).
Wojciechowski, R. & Hysi, P. G. Focusing in on the complex genetics of myopia. PLoS Genet. 9, e1003442 (2013).
Tedja, M. S. et al. Genome-wide association meta-analysis highlights light-induced signaling as a driver for refractive error. Nat. Genet. 50, 834–848 (2018).
Hysi, P. G. et al. Meta-analysis of 542,934 subjects of European ancestry identifies new genes and mechanisms predisposing to refractive error and myopia. Nat. Genet. 52, 401–407 (2020). The largest GWAS study to date in refractive error and myopia identifying 336 novel genetic loci.
Guggenheim, J. A. et al. Assumption-free estimation of the genetic contribution to refractive error across childhood. Mol. Vis. 21, 621–632 (2015).
Ghorbani Mojarrad, N. et al. Association between polygenic risk score and risk of myopia. JAMA Ophthalmol. 138, 7–13 (2019).
Tideman, J. W. L. et al. When do myopia genes have their effect? Comparison of genetic risks between children and adults. Genet. Epidemiol. 40, 756–766 (2016). This study demonstrated that different genes can impact on myopia at different ages.
Cheng, C. Y. et al. Nine loci for ocular axial length identified through genome-wide association studies, including shared loci with refractive error. Am. J. Hum. Genet. 93, 264–277 (2013). This study identified a number of genetic loci for axial length, including some that were shared with refractive error, using a large study cohort of the CREAM.
Hysi, P. G., Wojciechowski, R., Rahi, J. S. & Hammond, C. J. Genome-wide association studies of refractive error and myopia, lessons learned, and implications for the future. Investig. Ophthalmol. Vis. Sci. 55, 3344–3351 (2014).
Fan, Q. et al. Childhood gene-environment interactions and age-dependent effects of genetic variants associated with refractive error and myopia: the CREAM consortium. Sci. Rep. 6, 25853 (2016).
Chen, C.-J., Cohen, B. H. & Diamond, E. L. Genetic and environmental effects on the development of myopia in Chinese twin children. Ophthalmic Paediatr. Genet. 6, 113–119 (1985).
Saw, S.-M., Hong, C.-Y., Chia, K.-S., Stone, R. A. & Tan, D. Nearwork and myopia in young children. Lancet 357, 390 (2001).
Dudbridge, F. & Fletcher, O. Gene-environment dependence creates spurious gene-environment interaction. Am. J. Hum. Genet. 95, 301–307 (2014). An account of the conditions under which gene–environment dependence can arise, using as an example the potential interaction between a CYP3A variant and age at menarche on the risk of breast cancer.
Fan, Q. et al. Education influences the association between genetic variants and refractive error: a meta-analysis of five Singapore studies. Hum. Mol. Genet. 23, 546–554 (2014). A pioneering study reporting interactions between variants in SHISA6, GJD2 and ZMAT4 and level of education in determining susceptibility to myopia.
Wojciechowski, R., Yee, S. S., Simpson, C. L., Bailey-Wilson, J. E. & Stambolian, D. Matrix metalloproteinases and educational attainment in refractive error: evidence of gene–environment interactions in the age-related eye disease study. Ophthalmology 120, 298–305 (2012).
Tkatchenko, A. V. et al. APLP2 regulates refractive error and myopia development in mice and humans. PLoS Genet. 11, e1005432 (2015).
Chen, Y. P. et al. Selective breeding for susceptibility to myopia reveals a gene-environment interaction. Investig. Ophthalmol. Vis. Sci. 52, 4003–4011 (2011).
Pozarickij, A. et al. Quantile regression analysis reveals widespread evidence for gene-environment or gene-gene interactions in myopia development. Commun. Biol. 2, 167 (2019). A study suggesting that 88% of known GWAS loci for refractive error exhibit evidence of variance heterogeneity, which is a characteristic feature of involvement in a G×E interaction.
Huang, Y. et al. A genome-wide association study for susceptibility to visual experience-induced myopia. Invest. Ophthalmol. Vis. Sci. 60, 559–569 (2019).
Mutti, D. O. et al. Axial growth and changes in lenticular and corneal power during emmetropization in infants. Invest. Ophthalmol. Vis. Sci. 46, 3074–3080 (2005).
Ehrlich, D. L. et al. Infant emmetropization: longitudinal changes in refraction components from nine to twenty months of age. Optom. Vis. Sci. 74, 822–843 (1997).
Inagaki, Y. The rapid change of corneal curvature in the neonatal period and infancy. Arch. Ophthalmol. 104, 1026–1027 (1986).
Gordon, R. A. & Donzis, P. B. Refractive development of the human eye. Arch. Ophthalmol. 103, 785–789 (1985).
Fledelius, H. C. & Christensen, A. C. Reappraisal of the human ocular growth curve in fetal life, infancy, and early childhood. Br. J. Ophthalmol. 80, 918–921 (1996).
Saw, S. M. et al. Incidence and progression of myopia in Singaporean school children. Invest. Ophthalmol. Vis. Sci. 46, 51–57 (2005).
Mutti, D. O. et al. Corneal and crystalline lens dimensions before and after myopia onset. Optom. Vis. Sci. 89, 251–262 (2012).
Han, X., Guo, X., Lee, P. Y., Morgan, I. G. & He, M. Six-year changes in refraction and related ocular biometric factors in an adult Chinese population. PLoS ONE 12, e0183364 (2017).
Troilo, D. et al. IMI - report on experimental models of emmetropization and myopia. Invest. Ophthalmol. Vis. Sci. 60, M31–M88 (2019). This is the most recent and most comprehensive summary to date of the results obtained from studies of laboratory animals on the role of vision in the regulation of refractive development.
Schaeffel, F., Glasser, A. & Howland, H. C. Accommodation, refractive error and eye growth in chickens. Vis. Res. 28, 639–657 (1988).
Wallman, J. & Winawer, J. Homeostasis of eye growth and the question of myopia. Neuron 43, 447–468 (2004). This is the first comprehensive review of animal research on refractive development; it provides a unique perspective on how vision regulates ocular growth and refractive development.
Schaeffel, F. & Feldkaemper, M. P. Animal models in myopia research. Clin. Exp. Optom. 98, 507–517 (2015).
Arumugam, B., Hung, L.-F., To, C.-H., Holden, B. A. & Smith, E. L. 3rd The effects of simultaneous dual focus lenses on refractive development in infant monkeys. Investig. Ophthalmol. Vis. Sci. 55, 7423–7432 (2014).
Zhu, X. Temporal integration of visual signals in lens compensation (a review). Exp. Eye Res. 114, 69–76 (2013).
Tse, D. Y. & To, C.-H. Graded competing regional myopic and hyperopic defocus produce summated emmetropization set points in chicks. Investig. Ophthalmol. Vis. Sci. 52, 8056–8062 (2011).
McBrien, N. A. & Adams, D. W. A longitudinal investigation of adult-onset and adult-progression of myopia in an occupational group. Refractive and biometric findings. Invest. Ophthalmol. Vis. Sci. 38, 321–333 (1997).
Wallman, J., Gottlieb, M. D., Rajaram, V. & Fugate-Wentzek, L. Local retinal regions control local eye growth and myopia. Science 237, 73–77 (1987). This investigation demonstrated that ocular growth and refractive development are regulated by independent, local retinal mechanisms that operate in a regionally selective fashion, one of the most interesting and critical operational properties of the mechanisms that regulate refractive development.
Tkatchenko, T. V., Troilo, D., Benavente-Perez, A. & Tkatchenko, A. V. Gene expression in response to optical defocus of opposite signs reveals bidirectional mechanism of visually guided eye growth. PLoS Biol. 16, e2006021 (2018).
Fischer, A. J., McGuire, J. J., Schaeffel, F. & Stell, W. K. Light- and focus-dependent expression of the transcription factor ZENK in the chick retina. Nat. Neurosci. 2, 706–712 (1999).
Rucker, F. J. & Wallman, J. Cone signals for spectacle-lens compensation: differential responses to short and long wavelengths. Vis. Res. 48, 1980–1991 (2008).
Foulds, W. S., Barathi, V. A. & Luu, C. D. Progressive myopia or hyperopia can be induced in chicks and reversed by manipulation of the chromaticity of ambient light. Invest. Ophthalmol. Vis. Sci. 54, 8004–8012 (2013).
Hung, L. F., Arumugam, B., She, Z., Ostrin, L. & Smith, E. L. 3rd Narrow-band, long-wavelength lighting promotes hyperopia and retards vision-induced myopia in infant rhesus monkeys. Exp. Eye Res. 176, 147–160 (2018).
Hagen, L. A. et al. The association between L:M cone ratio, cone opsin genes and myopia susceptibility. Vis. Res. 162, 20–28 (2019).
Crewther, D. P. & Crewther, S. G. Refractive compensation to optical defocus depends on the temporal profile of luminance modulation of the environment. Neuroreport 13, 1029–1032 (2002).
Aleman, A. C., Wang, M. & Schaeffel, F. Reading and myopia: contrast polarity matters. Sci. Rep. 8, 10840 (2018).
Crewther, S. G. & Crewther, D. P. Inhibition of retinal ON/OFF systems differentially affects refractive compensation to defocus. Neuroreport 14, 1233–1237 (2003).
Chakraborty, R. et al. ON pathway mutations increase susceptibility to form-deprivation myopia. Exp. Eye Res. 137, 79–83 (2015).
Chakraborty, R. et al. Comparison of refractive development and retinal dopamine in OFF pathway mutant and C57BL/6J wild-type mice. Mol. Vis. 20, 1318–1327 (2014).
Wang, M., Aleman, A. C. & Schaeffel, F. Probing the potency of artificial dynamic ON or OFF stimuli to inhibit myopia development. Invest. Ophthalmol. Vis. Sci. 60, 2599–2611 (2019).
Chen, S. et al. Bright light suppresses form-deprivation myopia development with activation of dopamine D1 receptor signaling in the ON pathway in retina. Invest. Ophthalmol. Vis. Sci. 58, 2306–2316 (2017).
Zhang, Y. & Wildsoet, C. F. RPE and choroid mechanisms underlying ocular growth and myopia. Prog. Mol. Biol. Transl. Sci. 134, 221–240 (2015).
Rymer, J. & Wildsoet, C. F. The role of the retinal pigment epithelium in eye growth regulation and myopia: a review. Vis. Neurosci. 22, 251–261 (2005). It is likely that the retinal pigment epithelium plays a critical role in the signal cascade that regulates refractive development. This review provides a comprehensive summary of what is known about the pigment epithelium and vision-dependent refractive development.
Wallman, J. et al. Moving the retina: choroidal modulation of refractive state. Vis. Res. 35, 37–50 (1995).
Mertz, J. R. & Wallman, J. Choroidal retinoic acid synthesis: a possible mediator between refractive error and compensatory eye growth. Exp. Eye Res. 70, 519–527 (2000).
Wildsoet, C. & Wallman, J. Choroidal and scleral mechanisms of compensation for spectacle lenses in chicks. Vis. Res. 35, 1175–1194 (1995). This comprehensive study conclusively demonstrated that choroidal thickness was regulated by visual feedback and that changes in choroidal thickness could have a significant effect on the eye’s refractive state.
Siegwart, J. T. Jr & Norton, T. T. Regulation of the mechanical properties of tree shrew sclera by the visual environment. Vis. Res. 39, 387–407 (1999).
Rada, J. A., Nickla, D. L. & Troilo, D. Decreased proteoglycan synthesis associated with form deprivation myopia in mature primate eyes. Invest. Ophthalmol. Vis. Sci. 41, 2050–2058 (2000).
Siegwart, J. T. Jr & Norton, T. T. Selective regulation of MMP and TIMP mRNA levels in tree shrew sclera during minus lens compensation and recovery. Invest. Ophthalmol. Vis. Sci. 46, 3484–3492 (2005).
McBrien, N. A. & Gentle, A. Role of the sclera in the development and pathological complications of myopia. Prog. Retin. Eye Res. 22, 307–338 (2003).
Rada, J. A., Shelton, S. & Norton, T. T. The sclera and myopia. Exp. Eye Res. 82, 185–200 (2006). This paper reviewed the myopia-associated scleral extracellular matrix remodelling events during myopia progression in both experimental models and humans.
Wu, H. et al. Scleral hypoxia is a target for myopia control. Proc. Natl Acad. Sci. USA 115, e7091–e7100 (2018).
Zhang, S. et al. Changes in choroidal thickness and choroidal blood perfusion in guinea pig myopia. Invest. Ophthalmol. Vis. Sci. 60, 3074–3083 (2019). Scleral hypoxia can develop as a result of a decline in blood perfusion in the choroid. This paper documented that choroidal blood perfusion was significantly decreased in three models of guinea pig myopia.
Yang, Y. S. & Koh, J. W. Choroidal blood flow change in eyes with high myopia. Korean J. Ophthalmol. 29, 309–314 (2015). This paper reported a significant decrease of choroidal blood perfusion in highly myopic human eyes.
Shih, Y. F. et al. Ocular pulse amplitude in myopia. J. Ocul. Pharmacol. 7, 83–87 (1991).
Kniestedt, C. & Stamper, R. L. Visual acuity and its measurement. Ophthalmol. Clin. North Am. 16, 155–170 (2003).
Guo, X. et al. Normative distribution of visual acuity in 3- to 6-year-old Chinese preschoolers: the Shenzhen kindergarten eye study. Invest. Ophthalmol. Vis. Sci. 56, 1985–1992 (2015).
Anstice, N. S. & Thompson, B. The measurement of visual acuity in children: an evidence-based update. Clin. Exp. Optom. 97, 3–11 (2014).
Morgan, I. G., Iribarren, R., Fotouhi, A. & Grzybowski, A. Cycloplegic refraction is the gold standard for epidemiological studies. Acta Ophthalmol. 93, 581–585 (2015).
WHO. The impact of myopia and high myopia: report of the Joint World Health Organization–Brien Holden Vision Institute Global Scientific Meeting on Myopia, University of New South Wales, Sydney, Australia, 16–18 March 2015 (World Health Organization, 2017).
Negrel, A. D., Maul, E., Pokharel, G. P., Zhao, J. & Ellwein, L. B. Refractive error study in children: sampling and measurement methods for a multi-country survey. Am. J. Ophthalmol. 129, 421–426 (2000).
Wen, G. et al. Prevalence of myopia, hyperopia, and astigmatism in non-Hispanic white and Asian children: multi-ethnic pediatric eye disease study. Ophthalmology 120, 2109–2116 (2013).
Lee, J. H., Jee, D., Kwon, J. W. & Lee, W. K. Prevalence and risk factors for myopia in a rural Korean population. Invest. Ophthalmol. Vis. Sci. 54, 5466–5471 (2013).
Parssinen, O. The increased prevalence of myopia in Finland. Acta Ophthalmol. 90, 497–502 (2012).
Pan, C. W. et al. Variation in prevalence of myopia between generations of migrant indians living in Singapore. Am. J. Ophthalmol. 154, 376–381.e1 (2012).
Santodomingo-Rubido, J., Mallen, E. A. H., Gilmartin, B. & Wolffsohn, J. S. A new non-contact optical device for ocular biometry. Br. J. Ophthalmol. 86, 458–462 (2002).
Hussin, H. M., Spry, P. G., Majid, M. A. & Gouws, P. Reliability and validity of the partial coherence interferometry for measurement of ocular axial length in children. Eye 20, 1021–1024 (2006).
Curtin, B. J. & Karlin, D. B. Axial length measurements and fundus changes of the myopic eye. Am. J. Ophthalmol. 71, 42–53 (1971).
Miller, D. G. & Singerman, L. J. Natural history of choroidal neovascularization in high myopia. Curr. Opin. Ophthalmol. 12, 222–224 (2001).
Moriyama, M. et al. Topographic analyses of shape of eyes with pathologic myopia by high-resolution three-dimensional magnetic resonance imaging. Ophthalmology 118, 1626–1637 (2011). This study has established a novel technique — 3D MRI of the eye — to visualize the shape of the entire globe; an entire extent of posterior staphyloma becomes visible.
Guo, X. et al. Three-dimensional eye shape, myopic maculopathy, and visual acuity: the Zhongshan ophthalmic center-Brien Holden vision institute high myopia cohort study. Ophthalmology 124, 679–687 (2017).
Ohno-Matsui, K. & Jonas, J. B. Posterior staphyloma in pathologic myopia. Prog. Retin. Eye Res. 70, 99–109 (2019).
Ohno-Matsui, K. Proposed classification of posterior staphylomas based on analyses of eye shape by three-dimensional magnetic resonance imaging and wide-field fundus imaging. Ophthalmology 121, 1798–1809 (2014). Through the use of new techniques, 3D MRI and ultra-wide-field OCT, a novel classification has been established for posterior staphylomas.
Morgan, I. G., He, M. & Rose, K. A. Epidemic of pathologic myopia: what can laboratory studies and epidemiology tell us? Retina 37, 989–997 (2016).
Ohno-Matsui, K., Lai, T. Y. Y., Cheung, C. M. G. & Lai, C. C. Updates of pathologic myopia. Prog. Retin. Eye Res. 52, 156–187 (2016).
Ohno-Matsui, K. What is the fundamental nature of pathologic myopia? Retina 37, 1043–1048 (2016).
Yokoi, T. et al. Peripapillary diffuse chorioretinal atrophy in children as a sign of eventual pathologic myopia in adults. Ophthalmology 123, 1783–1787 (2016).
Ohno-Matsui, K. in Pathologic Myopia (eds Spaide, R. F., Ohno-Matsui, K., & Yannuzzi, L. A.) 187–210 (Springer, 2014).
Tong, L. et al. Screening for myopia and refractive errors using LogMAR visual acuity by optometrists and a simplified visual acuity chart by nurses. Optom. Vis. Sci. 81, 684–691 (2004).
Priya, A. et al. Vision screening by teachers in southern Indian schools: testing a new “all class teacher” model. Ophthalmic Epidemiol. 22, 60–65 (2015).
Sharma, A. et al. Strategies to improve the accuracy of vision measurement by teachers in rural Chinese secondary schoolchildren: Xichang Pediatric Refractive Error Study (X-PRES) report no. 6. Arch. Ophthalmol. 126, 1434–1440 (2008).
Pattison, B. & Plymat, K. Vision screening of school children: should it be continued? Contemp. Nurse 10, 163–171 (2001).
Ma, Y. et al. Myopia screening: combining visual acuity and noncycloplegic autorefraction. Optom. Vis. Sci. 90, 1479–1485 (2013).
Leone, J. F., Mitchell, P., Morgan, I. G., Kifley, A. & Rose, K. A. Use of visual acuity to screen for significant refractive errors in adolescents: is it reliable? Arch. Ophthalmol. 128, 894–899 (2010).
Tong, L. et al. Sensitivity and specificity of visual acuity screening for refractive errors in school children. Optom. Vis. Sci. 79, 650–657 (2002).
O’Donoghue, L., Rudnicka, A. R., McClelland, J. F., Logan, N. S. & Saunders, K. J. Visual acuity measures do not reliably detect childhood refractive error – an epidemiological study. PLoS ONE 7, e34441 (2012).
Lai, Y. H., Tseng, H. Y., Hsu, H. T., Chang, S. J. & Wang, H. Z. Uncorrected visual acuity and noncycloplegic autorefraction predict significant refractive errors in Taiwanese preschool children. Ophthalmology 120, 271–276 (2013).
Sherwin, J. C. et al. The association between time spent outdoors and myopia in children and adolescents: a systematic review and meta-analysis. Ophthalmology 119, 2141–2151 (2012).
Wu, P. C., Tsai, C. L., Wu, H. L., Yang, Y. H. & Kuo, H. K. Outdoor activity during class recess reduces myopia onset and progression in school children. Ophthalmology 120, 1080–1085 (2013).
Ngo, C. S. et al. A cluster randomised controlled trial evaluating an incentive-based outdoor physical activity programme to increase outdoor time and prevent myopia in children. Ophthalmic Physiol. Opt. 34, 362–368 (2014).
Jan, C. et al. Prevention of myopia, China. Bull. World Health Organ. 98, 435–437 (2020).
Chung, K., Mohidin, N. & O’Leary, D. J. Undercorrection of myopia enhances rather than inhibits myopia progression. Vis. Res. 42, 2555–2559 (2002). Undercorrection is widely practised in myopia management but this article showed that undercorrection worsened the progression of myopia.
Li, S. Y. et al. Effect of undercorrection on myopia progression in 12-year-old children. Graefes Arch. Clin. Exp. Ophthalmol. 253, 1363–1368 (2015).
Koomson, N. Y. et al. Relationship between reduced accommodative lag and myopia progression. Optom. Vis. Sci. 93, 683–691 (2016).
Walline, J. J., Greiner, K. L., McVey, M. E. & Jones-Jordan, L. A. Multifocal contact lens myopia control. Optom. Vis. Sci. 90, 1207–1214 (2013).
Cheng, D., Woo, G. C., Drobe, B. & Schmid, K. L. Effect of bifocal and prismatic bifocal spectacles on myopia progression in children: three-year results of a randomized clinical trial. JAMA Ophthalmol. 132, 258–264 (2014).
Cho, P. & Cheung, S. W. Retardation of myopia in Orthokeratology (ROMIO) study: a 2-year randomized clinical trial. Invest. Ophthalmol. Vis. Sci. 53, 7077–7085 (2012).
Edwards, M. H., Li, R. W.-H., Lam, C. S.-Y., Lew, J. K.-F. & Yu, B. S.-Y. The Hong Kong progressive lens myopia control study: study design and main findings. Invest. Ophthalmol. Vis. Sci. 43, 2852–2858 (2002).
Gwiazda, J. et al. A randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Invest. Ophthalmol. Vis. Sci. 44, 1492–1500 (2003).
Leung, J. T. & Brown, B. Progression of myopia in Hong Kong chinese schoolchildren is slowed by wearing progressive lenses. Optom. Vis. Sci. 76, 346–354 (1999).
Sankaridurg, P. et al. Spectacle lenses designed to reduce progression of myopia: 12-month results. Optom. Vis. Sci. 87, 631–641 (2010).
Anstice, N. S. & Phillips, J. R. Effect of dual-focus soft contact lens wear on axial myopia progression in children. Ophthalmology 118, 1152–1161 (2011). The study demonstrated the feasibility of slowing myopia with multifocal-type soft contact lenses.
Lam, C. S. Y., Tang, W. C., Tse, D. Y.-Y., Tang, Y. Y. & To, C. H. Defocus incorporated soft contact (DISC) lens slows myopia progression in Hong Kong Chinese schoolchildren: a 2-year randomised clinical trial. Br. J. Ophthalmol. 98, 40–45 (2014).
Walline, J. J., Jones, L. A. & Sinnott, L. T. Corneal reshaping and myopia progression. Br. J. Ophthalmol. 93, 1181–1185 (2009).
Cheng, X., Xu, J., Chehab, K., Exford, J. & Brennan, N. Soft contact lenses with positive spherical aberration for myopia control. Optom. Vis. Sci. 93, 353–366 (2016).
Sankaridurg, P. et al. Myopia control with novel central and peripheral plus contact lenses and extended depth of focus contact lenses: 2 year results from a randomised clinical trial. Ophthalmic Physiol. Opt. 39, 294–307 (2019).
Sankaridurg, P. et al. Decrease in rate of myopia progression with a contact lens designed to reduce relative peripheral hyperopia: one-year results. Invest. Ophthalmol. Vis. Sci. 52, 9362–9367 (2011). The study demonstrated the feasibility of slowing myopia with multifocal-type soft contact lenses.
Chamberlain, P. et al. A 3-year randomized clinical trial of MiSight lenses for myopia control. Optom. Vis. Sci. 96, 556–567 (2019).
Lam, C. S. Y. et al. Defocus incorporated multiple segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. Br. J. Ophthalmol. 104, 363–368 (2020).
Kanda, H. et al. Effect of spectacle lenses designed to reduce relative peripheral hyperopia on myopia progression in Japanese children: a 2-year multicenter randomized controlled trial. Jpn. J. Ophthalmol. 62, 537–543 (2018).
Walline, J. J. et al. Effect of high add power, medium add power, or single-vision contact lenses on myopia progression in children: the BLINK randomized clinical trial. JAMA 324, 571–580 (2020).
Walline, J. J. et al. Contact lenses in pediatrics (CLIP) study: chair time and ocular health. Optom. Vis. Sci. 84, 896–902 (2007).
Walline, J. J. et al. A randomized trial of the effect of soft contact lenses on myopia progression in children. Invest. Ophthalmol. Vis. Sci. 49, 4702–4706 (2008).
Gifford, K. L. et al. IMI - clinical management guidelines report. Invest. Ophthalmol. Vis. Sci. 60, M184–M203 (2019).
Berntsen, D. A., Sinnott, L. T., Mutti, D. O. & Zadnik, K. A randomized trial using progressive addition lenses to evaluate theories of myopia progression in children with a high lag of accommodation. Invest. Ophthalmol. Vis. Sci. 53, 640–649 (2012).
Stapleton, F. et al. The incidence of contact lens-related microbial keratitis in Australia. Ophthalmology 115, 1655–1662 (2008).
Ganesan, P. & Wildsoet, C. F. Pharmaceutical intervention for myopia control. Expert. Rev. Ophthalmol. 5, 759–787 (2010).
Pineles, S. L. et al. Atropine for the prevention of myopia progression in children: a report by the American Academy of Ophthalmology. Ophthalmology 124, 1857–1866 (2017).
Huang, J. et al. Efficacy comparison of 16 interventions for myopia control in children: a network meta-analysis. Ophthalmology 123, 697–708 (2016). This meta-analysis compared 16 different interventions for myopia control and indicated that, while a range of interventions could significantly reduce myopia progression, the most effective interventions were pharmacological such as atropine and pirenzepine.
Li, S. M. et al. Atropine slows myopia progression more in Asian than white children by meta-analysis. Optom. Vis. Sci. 91, 342–350 (2014). This meta-analysis of RCT results showed that atropine could significantly slow myopia progression in children with a greater effect in Asian children than in white children.
Gong, Q. et al. Efficacy and adverse effects of atropine in childhood myopia: a meta-analysis. JAMA Ophthalmol. 135, 624–630 (2017).
Chia, A. et al. Atropine for the treatment of childhood myopia: changes after stopping atropine 0.01%, 0.1% and 0.5%. Am. J. Ophthalmol. 157, 451–457.e1 (2014).
Chia, A., Lu, Q. S. & Tan, D. Five-year clinical trial on atropine for the treatment of myopia 2: myopia control with atropine 0.01% eyedrops. Ophthalmology 123, 391–399 (2016).
Fang, P. C., Chung, M. Y., Yu, H. J. & Wu, P. C. Prevention of myopia onset with 0.025% atropine in premyopic children. J. Ocul. Pharmacol. Ther. 26, 341–345 (2010).
Tong, L. et al. Atropine for the treatment of childhood myopia: effect on myopia progression after cessation of atropine. Ophthalmology 116, 572–579 (2009).
Yam, J. C. et al. Low-concentration atropine for myopia progression (LAMP) study: a randomized, double-blinded, placebo-controlled trial of 0.05%, 0.025%, and 0.01% atropine eye drops in myopia control. Ophthalmology 126, 113–124 (2019). This study showed that the use of very low concentrations of atropine eye drops could reduce myopia progression along a concentration-dependent response, with 0.05% atropine being the most effective in controlling SE progression and AL elongation over a period of 1 year.
Yam, J. C. et al. Two-year clinical trial of the low-concentration atropine for myopia progression (LAMP) study: phase 2 report. Ophthalmology 127, 910–919 (2019). Results of this 2-year randomized trial indicated that the effect of 0.05% atropine was double that observed with 0.01% atropine in slowing myopia progression.
Bedrossian, R. H. The effect of atropine on myopia. Ophthalmology 86, 713–719 (1979).
Yi, S. et al. Therapeutic effect of atropine 1% in children with low myopia. J. AAPOS 19, 426–429 (2015).
Chua, W. H. et al. Atropine for the treatment of childhood myopia. Ophthalmology 113, 2285–2291 (2006).
Shih, Y. F. et al. Effects of different concentrations of atropine on controlling myopia in myopic children. J. Ocul. Pharmacol. Ther. 15, 85–90 (1999). This study suggested that low concentrations of atropine at 0.1%, 0.25% and 0.5% showed significant effects on controlling myopia, with 0.5% atropine treatment being the most effective.
Lee, C. Y., Sun, C. C., Lin, Y. F. & Lin, K. K. Effects of topical atropine on intraocular pressure and myopia progression: a prospective comparative study. BMC Ophthalmol. 16, 114 (2016).
Wu, T. E., Yang, C. C. & Chen, H. S. Does atropine use increase intraocular pressure in myopic children? Optom. Vis. Sci. 89, E161–E167 (2012).
Chia, A., Li, W., Tan, D. & Luu, C. D. Full-field electroretinogram findings in children in the atropine treatment for myopia (ATOM2) study. Doc. Ophthalmol. 126, 177–186 (2013).
Luu, C. D., Lau, A. M., Koh, A. H. & Tan, D. Multifocal electroretinogram in children on atropine treatment for myopia. Br. J. Ophthalmol. 89, 151–153 (2005).
McBrien, N. A., Stell, W. K. & Carr, B. How does atropine exert its anti-myopia effects? Ophthalmic Physiol. Opt. 33, 373–378 (2013).
Kinoshita, N. et al. Additive effects of orthokeratology and atropine 0.01% ophthalmic solution in slowing axial elongation in children with myopia: first year results. Jpn. J. Ophthalmol. 62, 544–553 (2018).
Wan, L. et al. The synergistic effects of orthokeratology and atropine in slowing the progression of myopia. J. Clin. Med. 7, 259 (2018).
Kinoshita, N. et al. Efficacy of combined orthokeratology and 0.01% atropine solution for slowing axial elongation in children with myopia: a 2-year randomised trial. Sci. Rep. 10, 12750 (2020).
Clark, T. Y. & Clark, R. A. Atropine 0.01% eyedrops significantly reduce the progression of childhood myopia. J. Ocul. Pharmacol. Ther. 31, 541–545 (2015). This study showed that atropine at 0.01% could significantly reduce the rate of myopic progression over 1 year in children with minimal side effects.
Anderle, R. & Ventruba, J. The current state of refractive surgery. Coll. Antropol. 37 (Suppl. 1), 237–241 (2013). This article provides an overall view of refractive surgery.
Wen, D. et al. Postoperative efficacy, predictability, safety, and visual quality of laser corneal refractive surgery: a network meta-analysis. Am. J. Ophthalmol. 178, 65–78 (2017).
Kamiya, K. et al. A multicenter retrospective survey of refractive surgery in 78,248 eyes. J. Refract. Surg. 33, 598–602 (2017).
Yuen, L. H. et al. A 10-year prospective audit of LASIK outcomes for myopia in 37,932 eyes at a single institution in Asia. Ophthalmology 117, 1236–1244 e1231 (2010). This study demonstrates the efficacy, safety and predictability of LASIK.
Kezirian, G. M. & Stonecipher, K. G. Comparison of the IntraLase femtosecond laser and mechanical keratomes for laser in situ keratomileusis. J. Cataract Refract. Surg. 30, 804–811 (2004).
Rosman, M. et al. Comparison of efficacy and safety of laser in situ keratomileusis using 2 femtosecond laser platforms in contralateral eyes. J. Cataract Refract. Surg. 39, 1066–1073 (2013).
Zalentein, W. N., Tervo, T. M. & Holopainen, J. M. Seven-year follow-up of LASIK for myopia. J. Refract. Surg. 25, 312–318 (2009).
Giri, P. & Azar, D. T. Risk profiles of ectasia after keratorefractive surgery. Curr. Opin. Ophthalmol. 28, 337–342 (2017).
Wolle, M. A., Randleman, J. B. & Woodward, M. A. Complications of refractive surgery: ectasia after refractive surgery. Int. Ophthalmol. Clin. 56, 127–139 (2016).
Shortt, A. J. & Allan, B. D. Photorefractive keratectomy (PRK) versus laser-assisted in-situ keratomileusis (LASIK) for myopia. Cochrane Database Syst. Rev. 2, CD005135 (2006).
Matsumoto, J. C. & Chu, Y. S. Epi-LASIK update: overview of techniques and patient management. Int. Ophthalmol. Clin. 46, 105–115 (2006).
Sia, R. K., Coe, C. D., Edwards, J. D., Ryan, D. S. & Bower, K. S. Visual outcomes after Epi-LASIK and PRK for low and moderate myopia. J. Refract. Surg. 28, 65–71 (2012).
Kuryan, J., Cheema, A. & Chuck, R. S. Laser-assisted subepithelial keratectomy (LASEK) versus laser-assisted in-situ keratomileusis (LASIK) for correcting myopia. Cochrane Database Syst. Rev. 2, CD011080 (2017).
Naderi, M., Jadidi, K., Mosavi, S. A. & Daneshi, S. A. Transepithelial photorefractive keratectomy for low to moderate myopia in comparison with conventional photorefractive keratectomy. J. Ophthalmic Vis. Res. 11, 358–362 (2016).
Shortt, A. J., Allan, B. D. S. & Evans, J. R. Laser-assisted in-situ keratomileusis (LASIK) versus photorefractive keratectomy (PRK) for myopia. Cochrane Database Syst. Rev. 1, CD005135 (2013).
Santhiago, M. R., Netto, M. V. & Wilson, S. E. Mitomycin C: biological effects and use in refractive surgery. Cornea 31, 311–321 (2012).
Wallau, A. D. & Campos, M. Photorefractive keratectomy with mitomycin C versus LASIK in custom surgeries for myopia: a bilateral prospective randomized clinical trial. J. Refract. Surg. 24, 326–336 (2008).
Agca, A. et al. Refractive lenticule extraction (ReLEx) through a small incision (SMILE) for correction of myopia and myopic astigmatism: current perspectives. Clin. Ophthalmol. 10, 1905–1912 (2016). This article provides an overall view of SMILE.
Chan, C., Lawless, M., Sutton, G., Versace, P. & Hodge, C. Small incision lenticule extraction (SMILE) in 2015. Clin. Exp. Optom. 99, 204–212 (2016).
Cai, W. T. et al. Dry eye and corneal sensitivity after small incision lenticule extraction and femtosecond laser-assisted in situ keratomileusis: a Meta-analysis. Int. J. Ophthalmol. 10, 632–638 (2017).
Fernandez, J., Valero, A., Martinez, J., Pinero, D. P. & Rodriguez-Vallejo, M. Short-term outcomes of small-incision lenticule extraction (SMILE) for low, medium, and high myopia. Eur. J. Ophthalmol. 27, 153–159 (2017).
Kim, J. R., Kim, B. K., Mun, S. J., Chung, Y. T. & Kim, H. S. One-year outcomes of small-incision lenticule extraction (SMILE): mild to moderate myopia vs. high myopia. BMC Ophthalmol. 15, 59 (2015).
Osman, I. M., Helaly, H. A., Abdalla, M. & Shousha, M. A. Corneal biomechanical changes in eyes with small incision lenticule extraction and laser assisted in situ keratomileusis. BMC Ophthalmol. 16, 123 (2016).
Guell, J. L., Morral, M., Kook, D. & Kohnen, T. Phakic intraocular lenses part 1: historical overview, current models, selection criteria, and surgical techniques. J. Cataract Refract. Surg. 36, 1976–1993 (2010). This article provides an overall view of PIOL.
Lackner, B. et al. Long-term results of implantation of phakic posterior chamber intraocular lenses. J. Cataract Refract. Surg. 30, 2269–2276 (2004).
Perez-Cambrodi, R. J., Piñero, D. P., Ferrer-Blasco, T., Cerviño, A. & Brautaset, R. The posterior chamber phakic refractive lens (PRL): a review. Eye 27, 14–21 (2013).
Lee, J. et al. Long-term clinical results of posterior chamber phakic intraocular lens implantation to correct myopia. Clin. Exp. Ophthalmol. 44, 481–487 (2016).
Guerra, M. G. et al. Phakic intraocular lens implantation: refractive outcome and safety in patients with anterior chamber depth between 2.8 and 3.0 versus >/=3.0 mm. Ophthalmic Res. 57, 239–246 (2017).
AlSabaani, N. A. et al. Causes of phakic implantable collamer lens explantation/exchange at king khaled eye specialist hospital. Middle East Afr. J. Ophthalmol. 23, 293–295 (2016).
Fernandes, P. et al. Implantable collamer posterior chamber intraocular lenses: a review of potential complications. J. Refract. Surg. 27, 765–776 (2011).
Arne, J. L. Phakic intraocular lens implantation versus clear lens extraction in highly myopic eyes of 30- to 50-year-old patients. J. Cataract Refract. Surg. 30, 2092–2096 (2004).
Nanavaty, M. A. & Daya, S. M. Refractive lens exchange versus phakic intraocular lenses. Curr. Opin. Ophthalmol. 23, 54–61 (2012).
Basch, E. Patient-reported outcomes - harnessing patients’ voices to improve clinical care. N. Engl. J. Med. 376, 105–108 (2017).
Sensaki, S. et al. An ecologic study of trends in the prevalence of myopia in Chinese adults in Singapore born from the 1920s to 1980s. Ann. Acad. Med. Singap. 46, 229–236 (2017).
Coletta, N. J. & Watson, T. Effect of myopia on visual acuity measured with laser interference fringes. Vis. Res. 46, 636–651 (2006).
Mitchell, P., Hourihan, F., Sandbach, J. & Wang, J. J. The relationship between glaucoma and myopia: the Blue Mountains eye study. Ophthalmology 106, 2010–2015 (1999).
Polkinghorne, P. J. & Craig, J. P. Northern New Zealand rhegmatogenous retinal detachment study: epidemiology and risk factors. Clin. Exp. Ophthalmol. 32, 159–163 (2004).
Praveen, M. R., Vasavada, A. R., Jani, U. D., Trivedi, R. H. & Choudhary, P. K. Prevalence of cataract type in relation to axial length in subjects with high myopia and emmetropia in an Indian population. Am. J. Ophthalmol. 145, 176–181 (2008).
Tan, D., Tay, S. A., Loh, K. L. & Chia, A. Topical atropine in the control of myopia. Asia Pac. J. Ophthalmol. 5, 424–428 (2016).
Lamoureux, E. L. et al. The impact of corrected and uncorrected refractive error on visual functioning: the Singapore Malay eye study. Invest. Ophthalmol. Vis. Sci. 50, 2614–2620 (2009).
Kandel, H. et al. Uncorrected and corrected refractive error experiences of Nepalese adults: a qualitative study. Ophthalmic Epidemiol. 25, 147–161 (2018).
Ayaki, M., Torii, H., Tsubota, K. & Negishi, K. Decreased sleep quality in high myopia children. Sci. Rep. 6, 33902 (2016).
Rose, K. et al. Quality of life in myopia. Br. J. Ophthalmol. 84, 1031–1034 (2000).
Gwiazda, J. Treatment options for myopia. Optom. Vis. Sci. 86, 624–628 (2009).
Sutton, G., Lawless, M. & Hodge, C. Laser in situ keratomileusis in 2012: a review. Clin. Exp. Optom. 97, 18–29 (2014).
Uusitalo, R. J., Aine, E., Sen, N. H. & Laatikainen, L. Implantable contact lens for high myopia. J. Cataract Refract. Surg. 28, 29–36 (2002).
Markoulli, M. & Kolanu, S. Contact lens wear and dry eyes: challenges and solutions. Clin. Optom. 9, 41–48 (2017).
Shtein, R. M. Post-LASIK dry eye. Expert Rev. Ophthalmol. 6, 575–582 (2011).
Kandel, H., Khadka, J., Goggin, M. & Pesudovs, K. Impact of refractive error on quality of life: a qualitative study. Clin. Exp. Ophthalmol. 45, 677–688 (2017).
Van Der Wees, P. J. et al. Integrating the use of patient-reported outcomes for both clinical practice and performance measurement: views of experts from 3 countries. Milbank Q. 92, 754–775 (2014).
Pesudovs, K., Garamendi, E. & Elliott, D. B. The quality of life impact of refractive correction (QIRC) questionnaire: development and validation. Optom. Vis. Sci. 81, 769–777 (2004).
Berry, S., Mangione, C. M., Lindblad, A. S. & McDonnell, P. J. Development of the national eye institute refractive error correction quality of life questionnaire: focus groups. Ophthalmology 110, 2285–2291 (2003).
Vitale, S., Schein, O. D., Meinert, C. L. & Steinberg, E. P. The refractive status and vision profile: a questionnaire to measure vision-related quality of life in persons with refractive error. Ophthalmology 107, 1529–1539 (2000).
Kandel, H., Khadka, J., Goggin, M. & Pesudovs, K. Patient-reported outcomes for assessment of quality of life in refractive error: a systematic review. Optom. Vis. Sci. 94, 1102–1119 (2017). Comprehensive overview of current myopia-specific instruments and the shortcomings of each instrument, highlighting the current gap in myopia PROM assessment.
Cella, D., Gershon, R., Lai, J. S. & Choi, S. The future of outcomes measurement: item banking, tailored short-forms, and computerized adaptive assessment. Qual. Life Res. 16 (Suppl. 1), 133–141 (2007).
Gershon, R. C. Computer adaptive testing. J. Appl. Meas. 6, 109–127 (2005).
Baumhauer, J. F. & Bozic, K. J. Value-based healthcare: patient-reported outcomes in clinical decision making. Clin. Orthop. Relat. Res. 474, 1375–1378 (2016). This is a detailed look at how PROMs are becoming increasingly important in this era of value-based and personalized health care.
Hu, Y. et al. Association of age at myopia onset with risk of high myopia in adulthood in a 12-year follow-up of a Chinese cohort. JAMA Ophthalmol. https://doi.org/10.1001/jamaophthalmol.2020.3451 (2020).
Chia, A. et al. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (atropine for the treatment of myopia 2). Ophthalmology 119, 347–354 (2012).
Hyman, L. et al. Relationship of age, sex, and ethnicity with myopia progression and axial elongation in the correction of myopia evaluation trial. Arch. Ophthalmol. 123, 977–987 (2005).
Zhao, J. et al. The progression of refractive error in school-age children: Shunyi district, China. Am. J. Ophthalmol. 134, 735–743 (2002).
Chen, Y. et al. Contribution of genome-wide significant single nucleotide polymorphisms in myopia prediction: findings from a 10-year cohort of Chinese twin children. Ophthalmology 126, 1607–1614 (2019).
Lin, H. et al. Prediction of myopia development among Chinese school-aged children using refraction data from electronic medical records: a retrospective, multicentre machine learning study. PLoS Med. 15, e1002674 (2018).
Chen, Y., Zhang, J., Morgan, I. G. & He, M. Identifying children at risk of high myopia using population centile curves of refraction. PLoS ONE 11, e0167642 (2016).
Chua, S. Y. et al. Age of onset of myopia predicts risk of high myopia in later childhood in myopic Singapore children. Ophthalmic Physiol. Opt. 36, 388–394 (2016).
Zadnik, K. et al. Prediction of juvenile-onset myopia. JAMA Ophthalmol. 133, 683–689 (2015).
Tideman, J. W. L. et al. Axial length growth and the risk of developing myopia in european children. Acta Ophthalmol. 96, 301–309 (2018).
Verkicharla, P. K. et al. Development of the fitsight fitness tracker to increase time outdoors to prevent myopia. Transl. Vis. Sci. Technol. 6, 20 (2017).
Wen, L. et al. An objective comparison of light intensity and near-visual tasks between rural and urban school children in China by a wearable device Clouclip. Transl. Vis. Sci. Technol. 8, 15 (2019).
Lanca, C. & Saw, S. M. The association between digital screen time and myopia: a systematic review. Ophthalmic Physiol. Opt. 40, 216–229 (2020).
Smith, E. L. III Prentice award lecture 2010: a case for peripheral optical treatment strategies for myopia. Optometry Vis. Sci. 88, 1029–1044 (2011).
Acknowledgements
The authors thank Ian Morgan (Australian National University) for his tremendous help on preparing this manuscript. This study was supported by the Australian National Health and Medical Research Council (NHMRC) through project grant 1034329 and a Senior Research Fellowship (1138585 to P.N.B.); the National Medical Research Council (NRMC) Grant NMRC/CIRG/1446/2017 and A*STAR World Without Disease (Grant JRBMRR 151701) (S.-M.S. and C.L.); Clinician Scientist Award (Senior; NMRC/CSA-SI/0009/2016) (E.L.L.) and Transition Award (MOH-TA19may-0002) (R.M.); National Institutes of Health Grant EY-03611 and funds from the Brien Holden Vision Institute (E.L.S.); grants 81800860, 81422007 and 81371047 from the National Natural Science Foundation of China (X.Z.); Fight for Sight and Welsh Government Project Grant (Ref: 24WG201) (J.A.G.); and Fundamental Research Funds of the State Key Laboratory of Ophthalmology, the Research Accelerator Program at the University of Melbourne and the CERA Foundation in Australia (M.H.).
Author information
Authors and Affiliations
Contributions
Introduction (M.H., P.N.B. and J.A.G.); Epidemiology (S.-M.S., C.L., M.H., J.A.G. and P.N.B.); Mechanisms/Pathophysiology (M.H., P.N.B., J.A.G., E.L.S. and X.Z.); Diagnosis, screening and prevention (M.H. and K.-O.M.); Management (P.-C.W., P.S., A.C. and M.R.); Quality of life (E.L.L. and R.M.); Outlook (P.N.B., M.H. and J.A.G.); Overview of Primer (P.N.B. and M.H.).
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Peer review information
Nature Reviews Disease Primers thanks C. Leung, F. Schaeffel, K. Tsubota, T. Young and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Glossary
- Form deprivation myopia
-
Placing a diffusing filter in front of the eye.
- Myopic defocus
-
Image formed in front of retinal plane.
- Axial length
-
The distance from the anterior surface of the cornea to the retina.
- Hyperopic
-
Ability to focus on distant objects.
- Emmetropization
-
The development of the eye towards emmetropia, wherein the focus of distant objects is on the retina when the lens is in a relaxed state.
- Accommodation
-
The ability of the eye to change its focus from near to far.
- Hyperopic defocus
-
Blur resulting from the image formed behind the retinal plane.
- Choroid
-
A highly vascularized layer between the sclera and the retina.
- Cycloplegia
-
Paralysis of the ciliary muscles of the eye.
- Fundus
-
The interior surface of the back of the eye, comprising the retina, choroid and sclera.
- Indirect ophthalmoscopy
-
Examination to provide a wide view of the back of the eye using a beam of light and a hand-held lens.
- Staphyloma
-
Protrusion of a limited area of the posterior sclera.
- Choroidal neovascularization
-
The formation of new blood vessels in the choroid of the eye.
- Orthokeratology lenses
-
Rigid, gas-permeable lenses to flatten corneal curvature during overnight wear.
- Photophobia
-
Sensitivity to light.
- Excimer or femtosecond laser
-
A laser emitting concentrated light in the ultraviolet region of the spectrum.
- Phakic intraocular lens
-
(PIOL). Silicon or plastic lenses inserted into a person’s eye to restore vision but leaves the eye’s natural lens intact.
- Corneal ectasia
-
Abnormal change in shape of the cornea.
- Haze
-
A granular scarring of the corneal stroma due to inflammation.
- Corneal lenticule tissue
-
A small piece of corneal or synthetic material with a precise shape and thickness implanted into the cornea in order to change the corneal curvature.
- Infective endophthalmitis
-
Infection of the interior of the eye.
- Ocular biometry
-
Measurement of specific features that are common to the eye.
- Rasch analysis
-
A psychometric model for analysing categorical data, typically in the form of a questionnaire.
Rights and permissions
About this article

Cite this article
Baird, P.N., Saw, SM., Lanca, C. et al. Myopia. Nat Rev Dis Primers 6, 99 (2020). https://doi.org/10.1038/s41572-020-00231-4
Accepted:
Published:
DOI: https://doi.org/10.1038/s41572-020-00231-4
This article is cited by
-
Scleral remodeling during myopia development in mice eyes: a potential role of thrombospondin-1
Molecular Medicine (2024)
-
The influence of the environment and lifestyle on myopia
Journal of Physiological Anthropology (2024)
-
Association between weight-adjusted waist index and myopia in adolescents and young adults: results from NHANES 1999–2008
BMC Ophthalmology (2024)
-
Associations between corneal curvature and other anterior segment biometrics in young myopic adults
Scientific Reports (2024)
-
Eye morphometry, body size, and flexibility parameters in myopic adolescents
Scientific Reports (2024)